

Hypoxia in models of lung cancer: implications for targeted therapeutics
- PMID: 20858837
- PMCID: PMC2948600
- DOI: 10.1158/1078-0432.CCR-10-1206
Hypoxia in models of lung cancer: implications for targeted therapeutics
Abstract
Purpose: To efficiently translate experimental methods from bench to bedside, it is imperative that laboratory models of cancer mimic human disease as closely as possible. In this study, we sought to compare patterns of hypoxia in several standard and emerging mouse models of lung cancer to establish the appropriateness of each for evaluating the role of oxygen in lung cancer progression and therapeutic response.
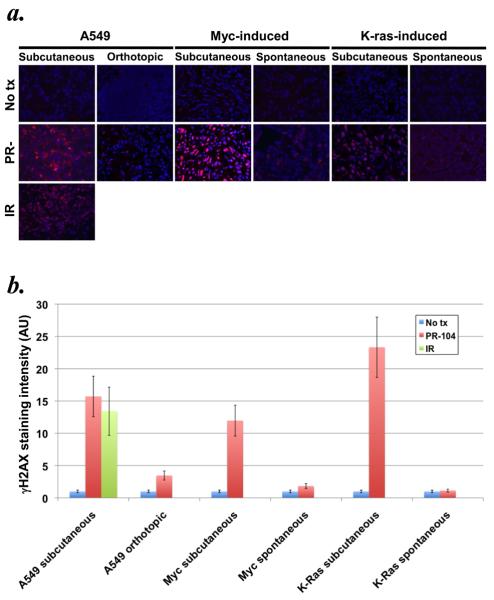
Experimental design: Subcutaneous and orthotopic human A549 lung carcinomas growing in nude mice as well as spontaneous K-ras or Myc-induced lung tumors grown in situ or subcutaneously were studied using fluorodeoxyglucose and fluoroazomycin arabinoside positron emission tomography, and postmortem by immunohistochemical observation of the hypoxia marker pimonidazole. The response of these models to the hypoxia-activated cytotoxin PR-104 was also quantified by the formation of γH2AX foci in vitro and in vivo. Finally, our findings were compared with oxygen electrode measurements of human lung cancers.
Results: Minimal fluoroazomycin arabinoside and pimonidazole accumulation was seen in tumors growing within the lungs, whereas subcutaneous tumors showed substantial trapping of both hypoxia probes. These observations correlated with the response of these tumors to PR-104, and with the reduced incidence of hypoxia in human lung cancers relative to other solid tumor types.
Conclusions: These findings suggest that in situ models of lung cancer in mice may be more reflective of the human disease, and encourage judicious selection of preclinical tumor models for the study of hypoxia imaging and antihypoxic cell therapies.
©2010 AACR.
Figures



Comment in
-
Location, location, location-makes all the difference for hypoxia in lung tumors.Clin Cancer Res. 2010 Oct 1;16(19):4685-7. doi: 10.1158/1078-0432.CCR-10-2004. Epub 2010 Sep 21. Clin Cancer Res. 2010. PMID: 20858842 Free PMC article.
References
-
- Gray LH, Conger AD, Ebert M, Hornsey S, Scott OCA. The concentration of oxygen dissolved in tissues at the time of irradiation as a factor in radiotherapy. British Journal of Radiology. 1953;26:638–48. - PubMed
-
- Höckel M, Vaupel P. Tumor Hypoxia: Definitions and Current Clinical, Biologic, and Molecular Aspects. Journal of the National Cancer Institute. 2001;93:266–76. - PubMed
-
- Brizel DM, Scully SP, Harrelson JM, et al. Tumor oxygenation predicts for the likelihood of distant metastases in human soft tissue sarcoma. Cancer Research. 1996;56:941–3. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
