

Self-management counseling in patients with heart failure: the heart failure adherence and retention randomized behavioral trial
- PMID: 20858878
- PMCID: PMC4097083
- DOI: 10.1001/jama.2010.1362
Self-management counseling in patients with heart failure: the heart failure adherence and retention randomized behavioral trial
Abstract
Context: Motivating patients with heart failure to adhere to medical advice has not translated into clinical benefit, but past trials have had methodological limitations.
Objective: To determine the value of self-management counseling plus heart failure education, compared with heart failure education alone, for the primary end point of death or heart failure hospitalization.
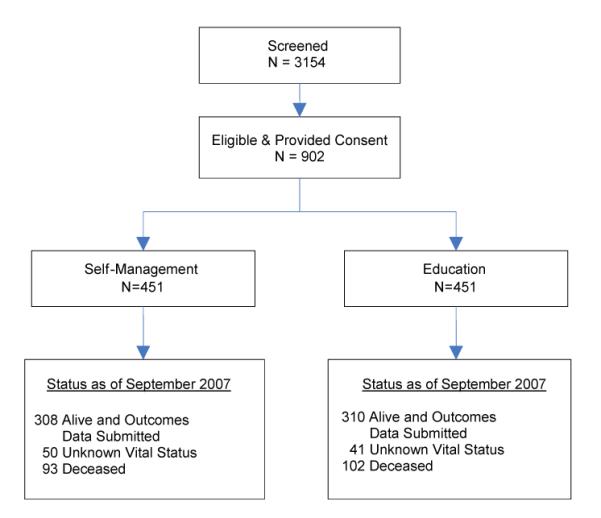
Design, setting, and patients: The Heart Failure Adherence and Retention Trial (HART), a single-center, multiple-hospital, partially blinded behavioral efficacy randomized controlled trial involving 902 patients with mild to moderate heart failure and reduced or preserved systolic function, randomized from the Chicago metropolitan area between October 2001 and October 2004 and undergoing follow-up for 2 to 3 subsequent years.
Interventions: All patients were offered 18 contacts and 18 heart failure educational tip sheets during the course of 1 year. Patients randomized to the education group received tip sheets in the mail and telephone calls to check comprehension. Patients randomized to the self-management group received tip sheets in groups and were taught self-management skills to implement the advice.
Main outcome measure: Death or heart failure hospitalization during a median of 2.56 years of follow-up.
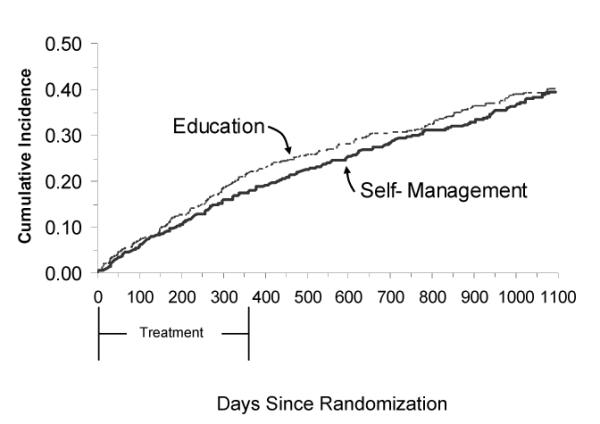
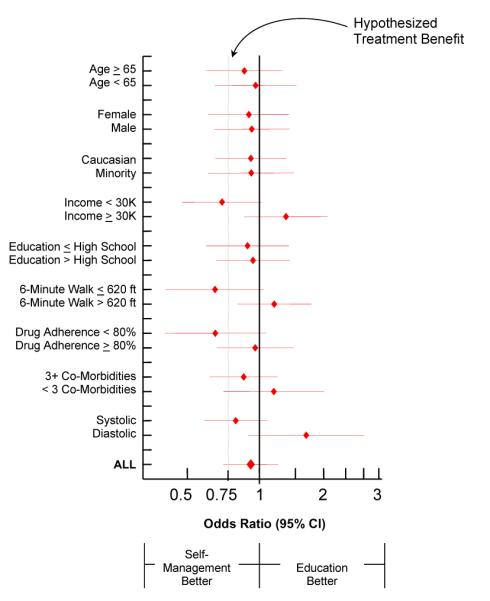
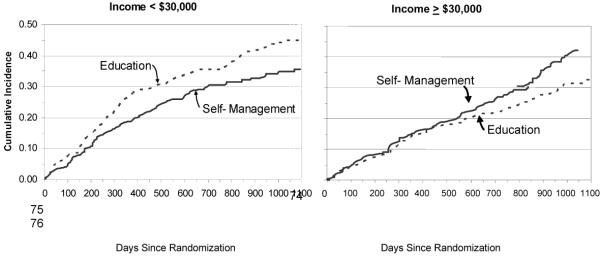
Results: Patients were representative of typical clinical populations (mean age, 63.6 years; 47% women, 40% racial/ethnic minority, 52% with annual family income less than $30,000, and 23% with preserved systolic function). The rate of the primary end point in the self-management group was no different from that in the education group (163 [40.1%)] vs 171 [41.2%], respectively; odds ratio, 0.95 [95% confidence interval, 0.72-1.26]). There were no significant differences on any secondary end points, including death, heart failure hospitalization, all-cause hospitalization, or quality of life.
Conclusions: Compared with an enhanced educational intervention alone, the addition of self-management counseling did not reduce death or heart failure hospitalization in patients with mild to moderate heart failure.
Trial registration: clinicaltrials.gov Identifier: NCT00018005.
Figures
Comment in
-
Enlisting the help of the largest health care workforce--patients.JAMA. 2010 Sep 22;304(12):1383-4. doi: 10.1001/jama.2010.1387. JAMA. 2010. PMID: 20858885 No abstract available.
References
-
- McCullough PA, Philbin EF, Spertus JA, et al. Confirmation of a heart failure epidemic: findings from the resource utilization among congestive heart failure (REACH) study. J Am Coll Cardiol. 2002;39:60–69. - PubMed
-
- Aghababian RV. Acutely decompensated heart failure: opportunities to improve care and outcomes in the emergency department. Rev Cardiovasc Med. 2002;3(suppl 4):S3–S9. - PubMed
-
- Russo CA, Ho K, Elixhauser A. HCUP Statistical Brief #26. Agency for Healthcare Research and Quality; Rockville, MD: Feb, 2007. Hospital stays for circulatory diseases, 2004. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb26.pdf. - PubMed
-
- Massie BM, Shah NB. Evolving trends in the epidemiologic factors of heart failure: rationale for preventive strategies and comprehensive disease management. Am Heart J. 1997;133:703–712. - PubMed
-
- Rosamond W, Flegal K, Friday G, et al. Heart disease and stroke statistics—2007 Update. A report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2007;115:e69–3171. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
