

Quality concerns with routine alcohol screening in VA clinical settings
- PMID: 20859699
- PMCID: PMC3043188
- DOI: 10.1007/s11606-010-1509-4
Quality concerns with routine alcohol screening in VA clinical settings
Abstract
Background: Alcohol screening questionnaires have typically been validated when self- or researcher-administered. Little is known about the performance of alcohol screening questionnaires administered in clinical settings.
Objective: The purpose of this study was to compare the results of alcohol screening conducted as part of routine outpatient clinical care in the Veterans Affairs (VA) Health Care System to the results on the same alcohol screening questionnaire completed on a mailed survey within 90 days and identify factors associated with discordant screening results.
Design: Cross sectional.
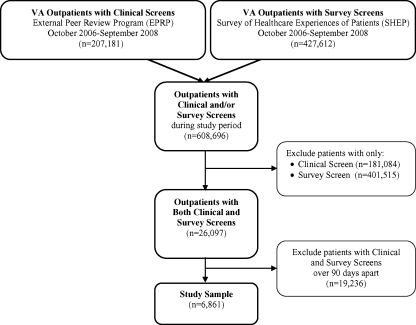
Participants: A national sample of 6,861 VA outpatients (fiscal years 2007-2008) who completed the AUDIT-C alcohol screening questionnaire on mailed surveys (survey screen) within 90 days of having clinical AUDIT-C screening documented in their medical records (clinical screen).
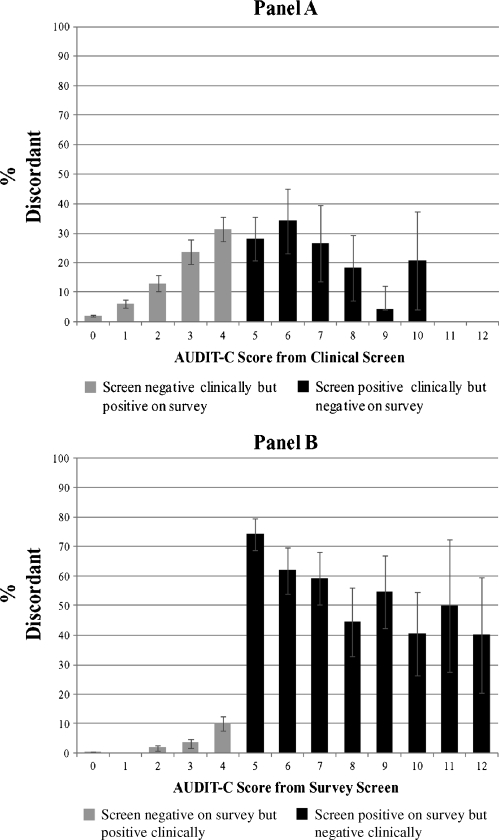
Main measures: Alcohol screening results were considered discordant if patients screened positive (AUDIT-C ≥ 5) on either the clinical or survey screen but not both. Multivariable logistic regression was used to estimate the prevalence of discordance in different patient subgroups based on demographic and clinical characteristics, VA network and temporal factors (e.g. the order of screens).
Key results: Whereas 11.1% (95% CI 10.4-11.9%) of patients screened positive for unhealthy alcohol use on the survey screen, 5.7% (5.1- 6.2%) screened positive on the clinical screen. Of 765 patients who screened positive on the survey screen, 61.2% (57.7-64.6%) had discordant results on the clinical screen, contrasted with 1.5% (1.2-1.8%) of 6096 patients who screened negative on the survey screen. In multivariable analyses, discordance was significantly increased among Black patients compared with White, and among patients who had a positive survey AUDIT-C screen or who received care at 4 of 21 VA networks.
Conclusion: Use of a validated alcohol screening questionnaire does not-by itself-ensure the quality of alcohol screening. This study suggests that the quality of clinical alcohol screening should be monitored, even when well-validated screening questionnaires are used.
Figures
References
-
- Room R, Babor T, Rehm J. Alcohol and public health. Lancet. 2005;365(9458):519–530. - PubMed
-
- Whitlock EP, Polen MR, Green CA, Orleans T, Klein J. Behavioral counseling interventions in primary care to reduce risky/harmful alcohol use by adults: A summary of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2004;140:557–568. - PubMed
-
- Kaner E, Beyer F, Dickinson H, et al. Effectiveness of brief alcohol interventions in primary care populations. Cochrane Database Syst Rev. 2007;(2):CD004148. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
