

An update on androgen deprivation therapy for prostate cancer
- PMID: 20861285
- PMCID: PMC3461824
- DOI: 10.1677/ERC-10-0187
An update on androgen deprivation therapy for prostate cancer
Abstract
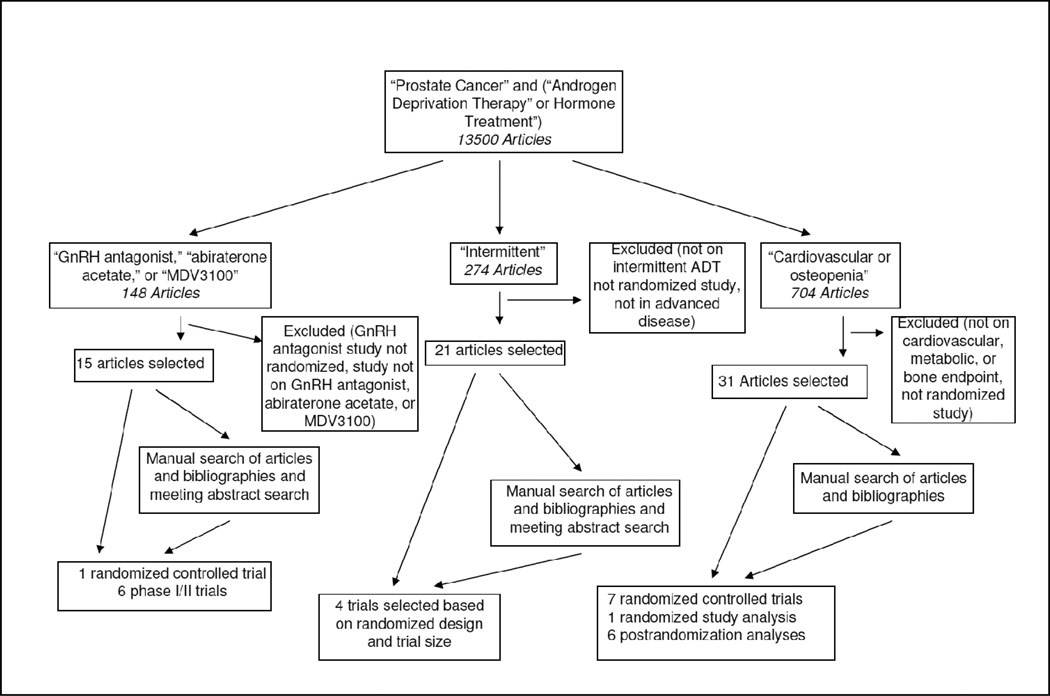
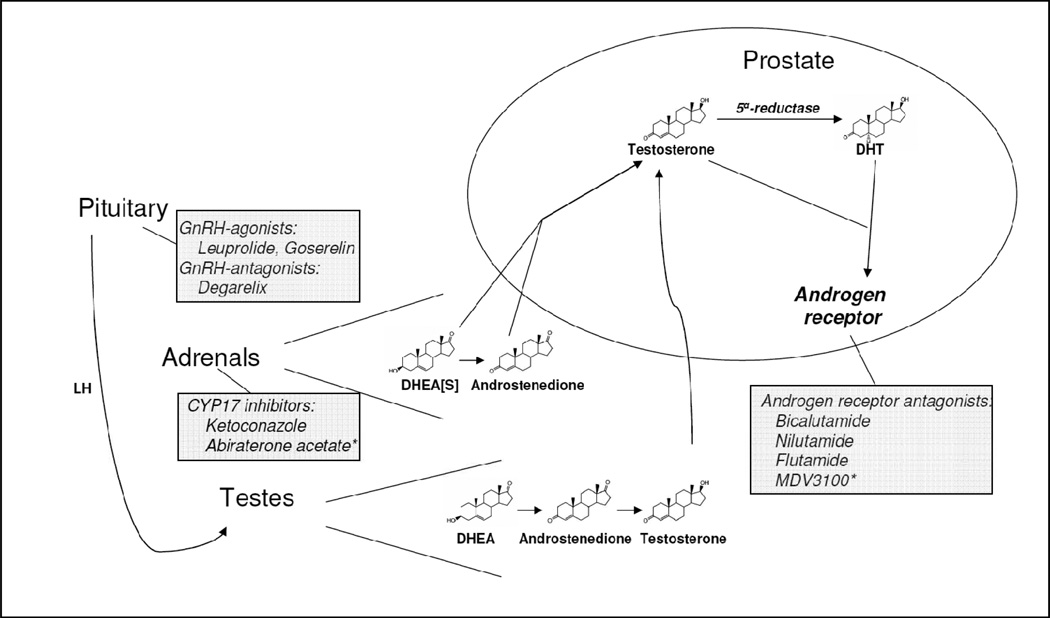
Androgen deprivation therapy (ADT) with gonadal testosterone depletion is the frontline treatment for advanced prostate cancer. Other hormonal interventions have a role in the treatment of prostate cancer. We sought to examine systematically the evidence for hormonal interventions in prostate cancer, risks of ADT, and interventions that mitigate these risks. Search results for therapeutic studies were focused primarily on randomized controlled clinical trials, and the Jadad scale criteria were used to evaluate the quality of these studies. Four trials of the efficacy of intermittent ADT versus continuous ADT were included. One randomized study analysis and six postrandomization analyses were included on the effects of ADT on cardiovascular mortality. Seven randomized controlled trials of pharmacologic interventions were included for the treatment of metabolic effects due to ADT. One randomized trial of GnRH antagonist versus GnRH agonist was included. Six phase I/II clinical trials of secondary hormonal therapies with novel mechanisms of action were included. Randomized studies completed to date indicate that intermittent ADT might be equivalent to continuous ADT. Although adverse effects of ADT include risk factors for cardiovascular disease, effects on cardiovascular mortality are uncertain. Bone loss and increased risk of fracture may be effectively treated with pharmacologic interventions. Benefits of ADT must be balanced with a consideration of the risks.
Conflict of interest statement
Figures
References
-
- Immediate versus deferred treatment for advanced prostatic cancer: initial results of the Medical Research Council Trial. The Medical Research Council Prostate Cancer Working Party Investigators Group. Br J Urol. 1997;79:235–246. - PubMed
-
- Akakura K, Bruchovsky N, Goldenberg SL, Rennie PS, Buckley AR, Sullivan LD. Effects of intermittent androgen suppression on androgen-dependent tumors. Apoptosis and serum prostate-specific antigen. Cancer. 1993;71:2782–2790. - PubMed
-
- Attard G, Reid AH, Yap TA, Raynaud F, Dowsett M, Settatree S, Barrett M, Parker C, Martins V, Folkerd E, et al. Phase I clinical trial of a selective inhibitor of CYP17, abiraterone acetate, confirms that castration-resistant prostate cancer commonly remains hormone driven. J Clin Oncol. 2008;26:4563–4571. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
