

The influence of pre-existing diabetes mellitus on the host immune response and outcome of pneumonia: analysis of two multicentre cohort studies
- PMID: 20861291
- PMCID: PMC3306240
- DOI: 10.1136/thx.2010.136317
The influence of pre-existing diabetes mellitus on the host immune response and outcome of pneumonia: analysis of two multicentre cohort studies
Abstract
Background: Although diabetes mellitus is implicated in susceptibility to infection, the association of diabetes with the subsequent course and outcome is unclear.
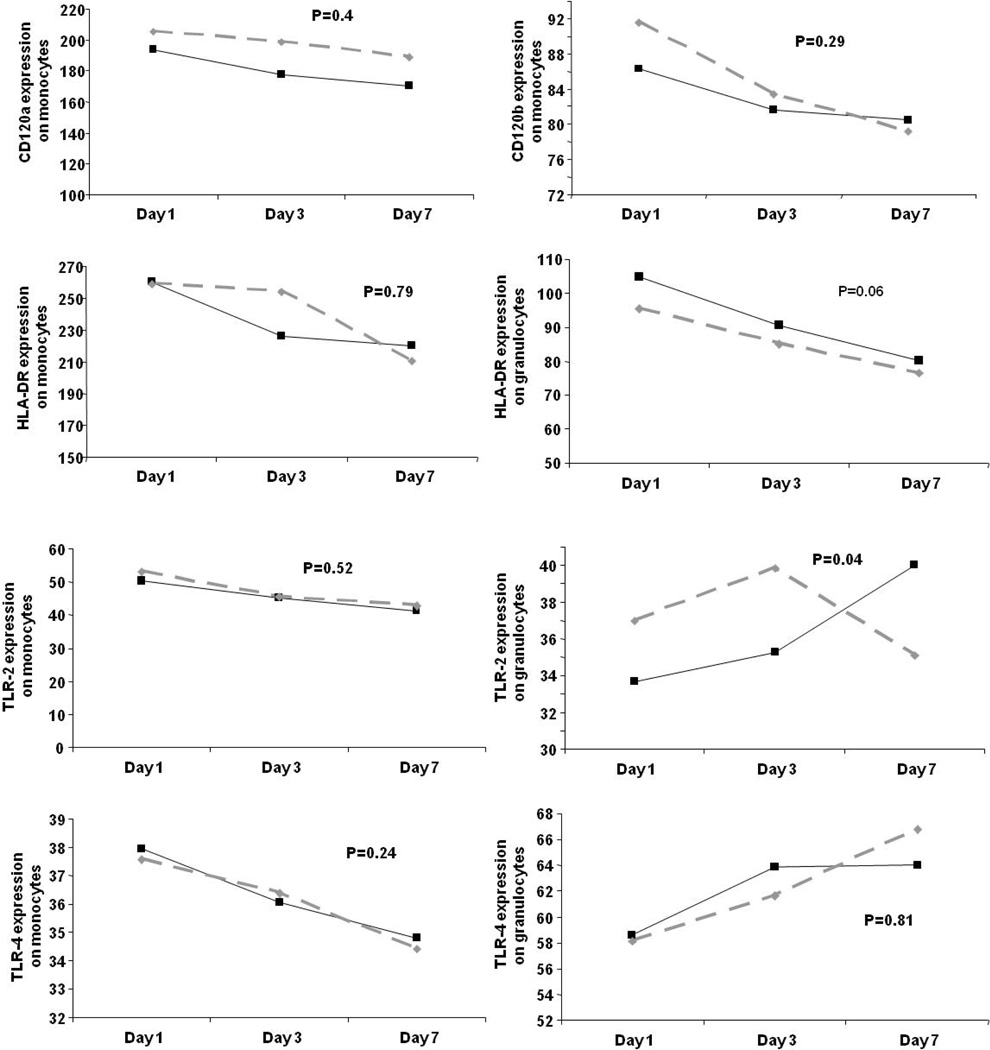
Methods: A retrospective analysis of two multicentre cohorts was carried out. The effect of pre-existing diabetes on the host immune response, acute organ function and mortality in patients hospitalised with community-acquired pneumonia (CAP) in the GenIMS study (n=1895) and on mortality following either CAP or non-infectious hospitalisations in the population-based cohort study, Health ABC (n=1639) was determined. Measurements included the mortality rate within the first year, risk of organ dysfunction, and immune responses, including circulating inflammatory (tumour necrosis factor, interleukin 6, interleukin 10), coagulation (Factor IX, thrombin-antithrombin complexes, antithrombin), fibrinolysis (plasminogen-activator inhibitor-1 and D-dimer) and cell surface markers (CD120a, CD120b, human leucocyte antigen (HLA)-DR, Toll-like receptor-2 and Toll-like receptor-4).
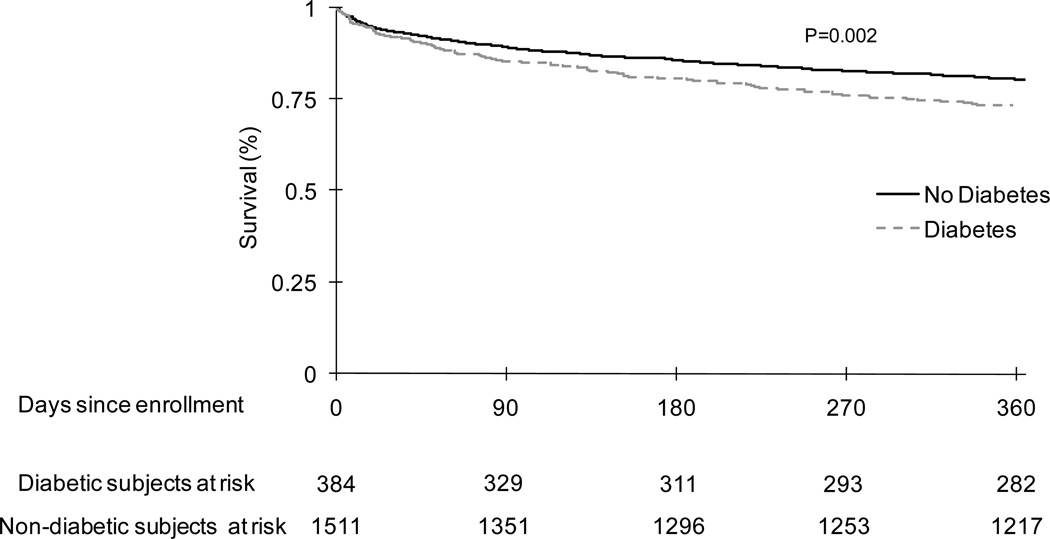
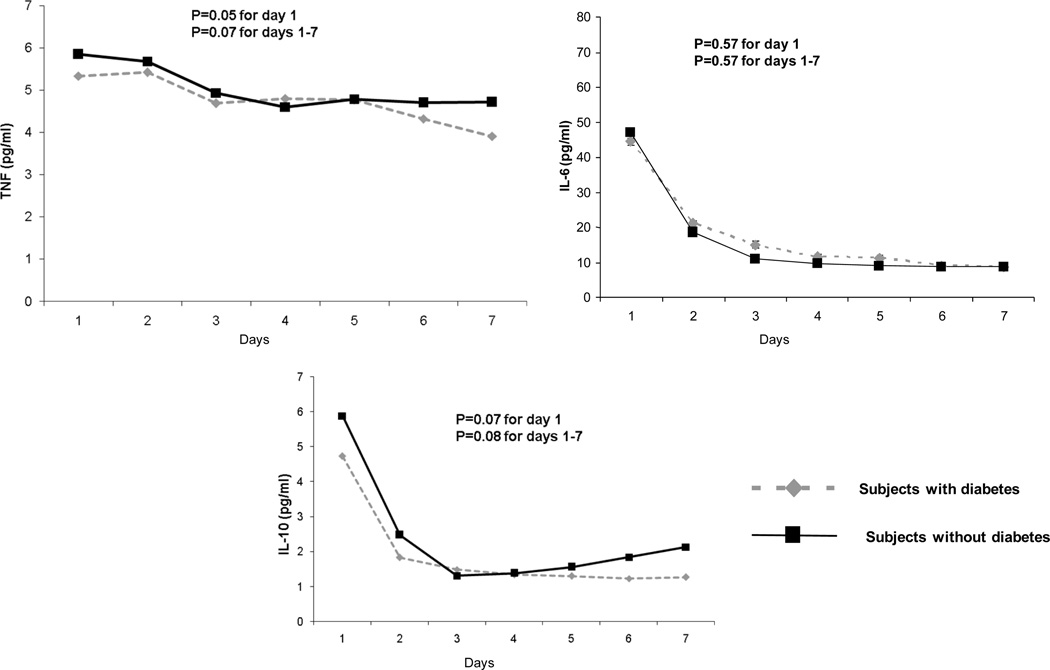
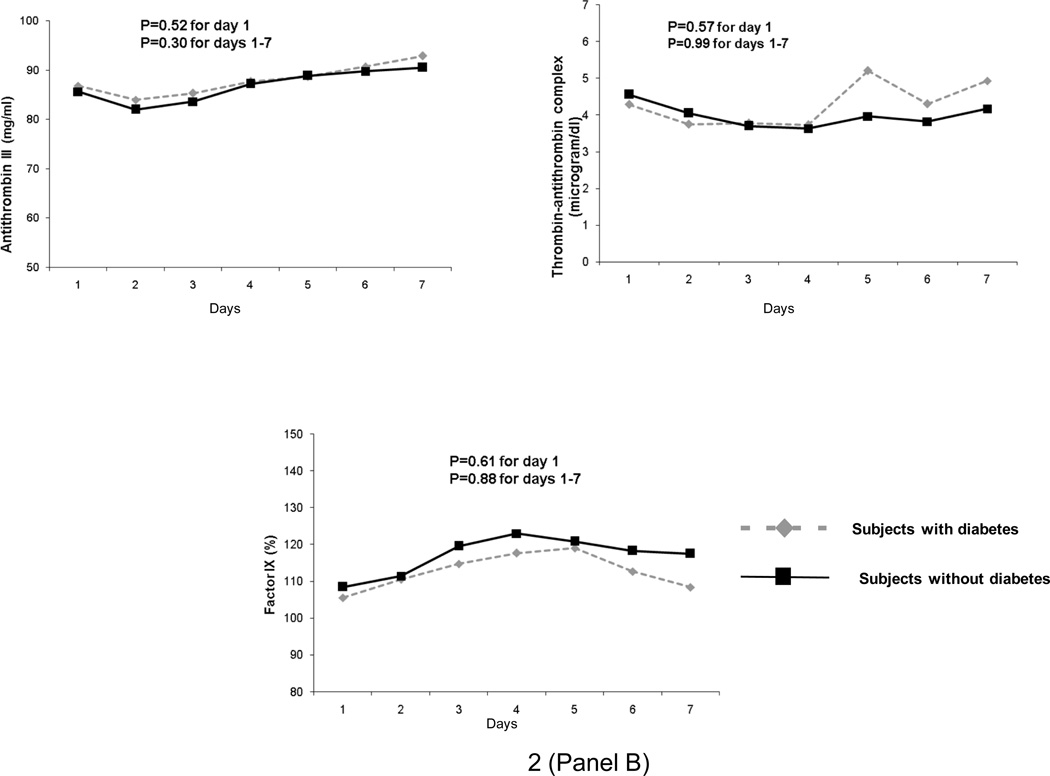
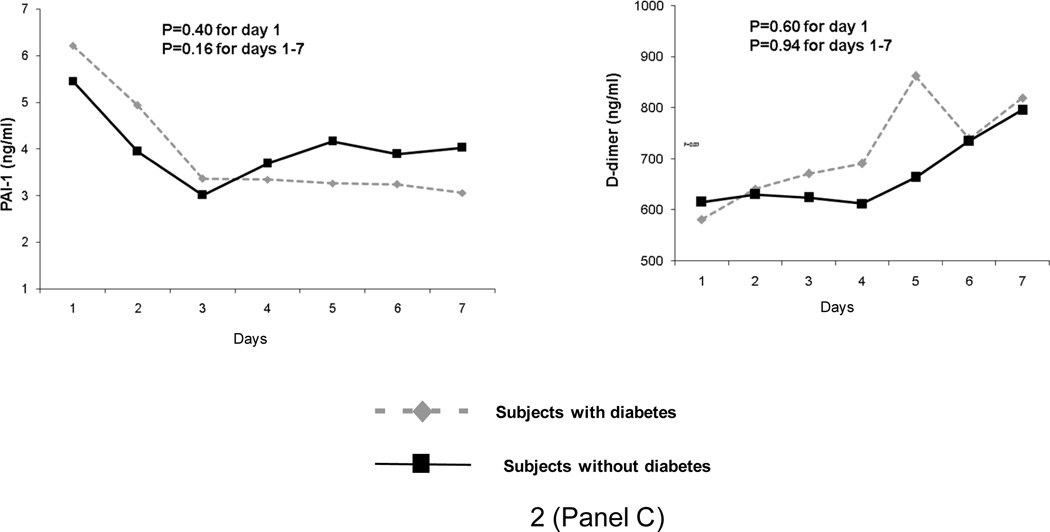
Results: In GenIMS, diabetes increased the mortality rate within the first year after CAP (unadjusted HR 1.41, 95% CI 1.12 to 1.76, p=0.002), even after adjusting for pre-existing cardiovascular and renal disease (adjusted HR 1.3, 95% CI 1.03 to 1.65, p=0.02). In Health ABC, diabetes increased the mortality rate within the first year following CAP hospitalisation, but not after hospitalisation for non-infectious illnesses (significant interaction for diabetes and reason for hospitalisation (p=0.04); HR for diabetes on mortality over the first year after CAP 1.87, 95% CI 0.76 to 4.6, p=0.16, and after non-infectious hospitalisation 1.16, 95% CI 0.8 to 1.6, p=0.37). In GenIMS, immediate immune response was similar, as evidenced by similar circulating immune marker levels, in the emergency department and during the first week. Those with diabetes had a higher risk of acute kidney injury during hospitalisation (39.3% vs 31.7%, p=0.005) and they were more likely to die due to cardiovascular and kidney disease (34.4% vs 26.8% and 10.4% vs 4.5%, p=0.03).
Conclusions: Pre-existing diabetes was associated with a higher risk of death following CAP. The mechanism is not due to an altered immune response, at least as measured by a broad panel of circulating and cell surface markers, but may be due to worsening of pre-existing cardiovascular and kidney disease.
Figures
References
-
- Shah BR, Hux JE. Quantifying the risk of infectious diseases for people with diabetes. Diabetes Care. 2003;26(2):510–513. - PubMed
-
- Muller LM, Gorter KJ, Hak E, et al. Increased risk of common infections in patients with type 1 and type 2 diabetes mellitus. Clin Infect Dis. 2005;41(3):281–288. - PubMed
-
- Falguera M, Pifarre R, Martin A, et al. Etiology and outcome of community-acquired pneumonia in patients with diabetes mellitus. Chest. 2005;128(5):3233–3239. - PubMed
-
- Kornum JB, Thomsen RW, Riis A, et al. Type 2 diabetes and pneumonia outcomes: A population-based cohort study. Diabetes Care. 2007;30(9):2251–2257. - PubMed
-
- Benfield T, Jensen JS, Nordestgaard BG. Influence of diabetes and hyperglycaemia on infectious disease hospitalisation and outcome. Diabetologia. 2007;50(3):549–554. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous