

Standardised pre-hospital care of acute myocardial infarction patients: MISSION! guidelines applied in practice
- PMID: 20862235
- PMCID: PMC2941126
- DOI: 10.1007/BF03091807
Standardised pre-hospital care of acute myocardial infarction patients: MISSION! guidelines applied in practice
Abstract
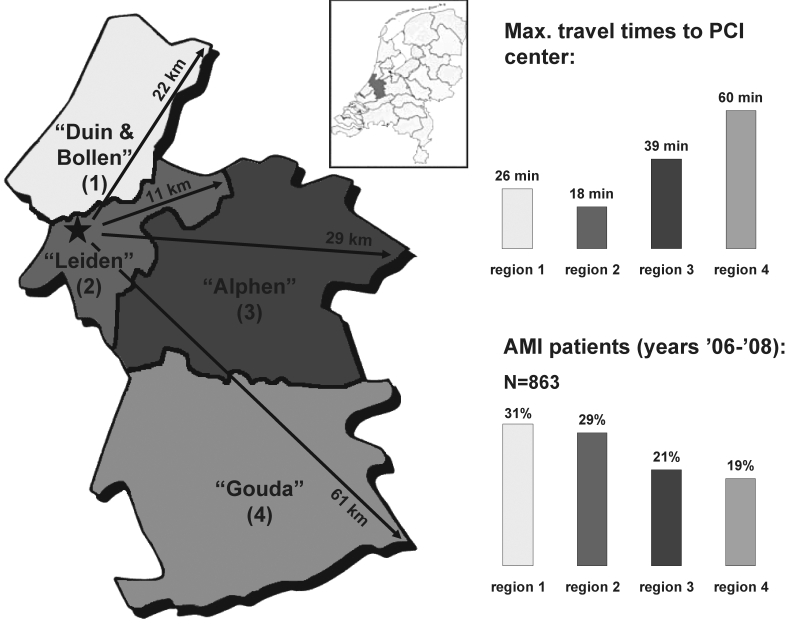
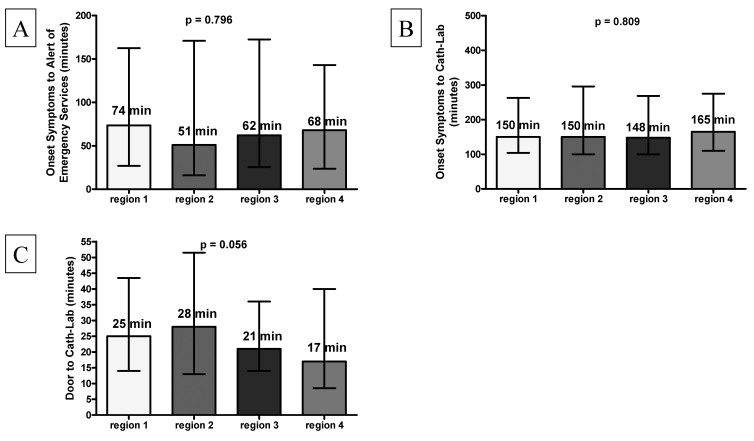
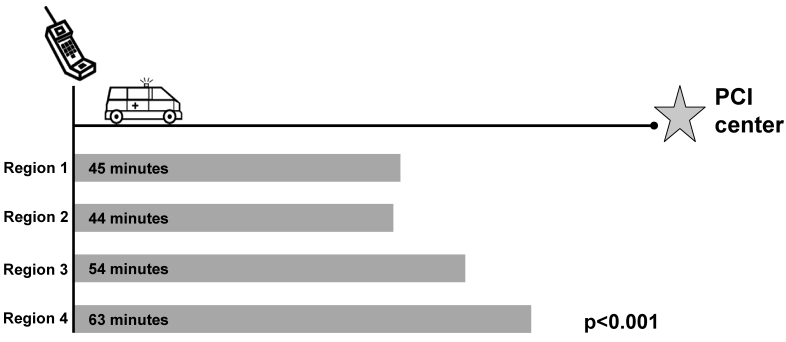
Background. To improve acute myocardial infarction (AMI) care in the region 'Hollands-Midden' (the Netherlands), a standardised guideline-based care program was developed (MISSION!). This study aimed to evaluate the outcome of the pre-hospital part of the MISSION! program and to study potential differences in pre-hospital care between four areas of residency.Methods. Time-to-treatment delays, AMI risk profile, cardiac enzymes, hospital stay, in-hospital mortality, and pre-AMI medication was evaluated in consecutive AMI patients (n=863, 61±13years, 75% male) transferred to the Leiden University Medical Center for primary percutaneous coronary intervention (PCI).Results. Median time interval between onset of symptoms and arrival at the catheterisation laboratory was 150 (interquartile range [IQR] 101-280) minutes. The alert of emergency services to arrival at the hospital time was 48 (IQR 40-60) minutes and the door-to-catheterisation laboratory time was 23 (IQR 13-42) minutes. Despite significant regional differences in ambulance transportation times no difference in total time from onset of symptoms to arrival at the catheterisation room was found. Peak troponin T was 3.33 (IQR 1.23-7.04) μg/l, hospital stay was 2 (IQR 2-3) days and in-hospital mortality was 2.3%. Twelve percent had 0 known risk factors, 30% had one risk factor, 45% two to three risk factors and 13% had four or more risk factors. No significant differences were observed for AMI risk profiles and medication pre-AMI. Conclusions. This study shows that a standardised regional AMI treatment protocol achieved optimal and uniformly distributed pre-hospital performance in the region 'Hollands-Midden', resulting in minimal time delays regardless of area of residence. Hospital stay was short and in-hospital mortality low. Of the patients, 88% had ≥1 modifiable risk factor. (Neth Heart J 2010;18:408-15.).
Keywords: Angioplasty, Transluminal, Percutaneous Coronary; Myocardial Infarction/therapy; Prevention & Control; Time Factors.
Figures
References
-
- Antman EM, Hand M, Armstrong PW, Bates ER, Green LA, Halasyamani LK, et al. 2007 Focused Update of the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines: developed in collaboration With the Canadian Cardiovascular Society endorsed by the American Academy of Family Physicians: 2007 Writing Group to Review New Evidence and Update the ACC/AHA 2004 Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction, Writing on Behalf of the 2004 Writing Committee. Circulation. 2008;117:296-329. - PubMed
-
- Van de Werf F, Ardissino D, Betriu A, Cokkinos DV, Falk E, Fox KA, et al. Management of acute myocardial infarction in patients presenting with ST-segment elevation. The Task Force on the Management of Acute Myocardial Infarction of the European Society of Cardiology. Eur Heart J. 2003;24:28-66. - PubMed
-
- van der Meulen A. Sterfte aan hart- en vaatziekten sinds 1970 gehalveerd; bron: Statistics Netherlands. 2005.
-
- Hunink MG, Goldman L, Tosteson AN, Mittleman MA, Goldman PA, Williams LW, et al. The recent decline in mortality from coronary heart disease, 1980-1990. The effect of secular trends in risk factors and treatment. JAMA. 1997;277:535-42. - PubMed
-
- McGovern PG, Pankow JS, Shahar E, Doliszny KM, Folsom AR, Blackburn H, et al. Recent trends in acute coronary heart disease--mortality, morbidity, medical care, and risk factors. The Minnesota Heart Survey Investigators. N Engl J Med. 1996;334:884-90. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous