

Cost-effectiveness of a central venous catheter care bundle
- PMID: 20862246
- PMCID: PMC2941454
- DOI: 10.1371/journal.pone.0012815
Cost-effectiveness of a central venous catheter care bundle
Abstract
Background: A bundled approach to central venous catheter care is currently being promoted as an effective way of preventing catheter-related bloodstream infection (CR-BSI). Consumables used in the bundled approach are relatively inexpensive which may lead to the conclusion that the bundle is cost-effective. However, this fails to consider the nontrivial costs of the monitoring and education activities required to implement the bundle, or that alternative strategies are available to prevent CR-BSI. We evaluated the cost-effectiveness of a bundle to prevent CR-BSI in Australian intensive care patients.
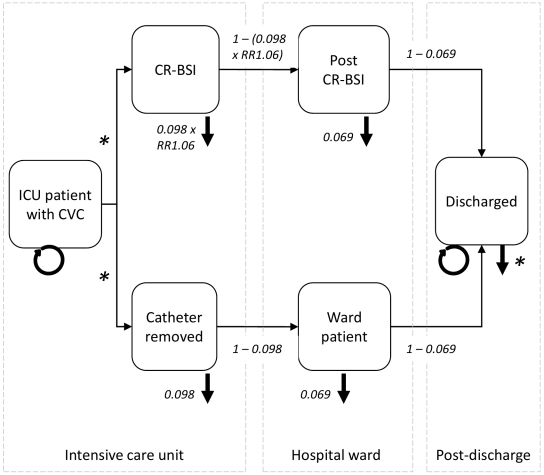
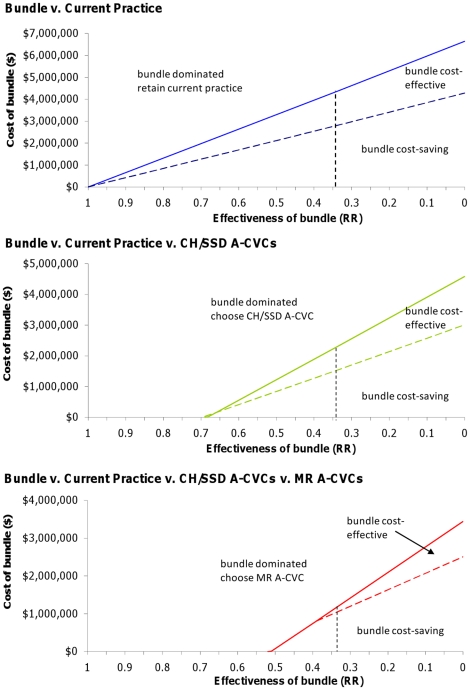
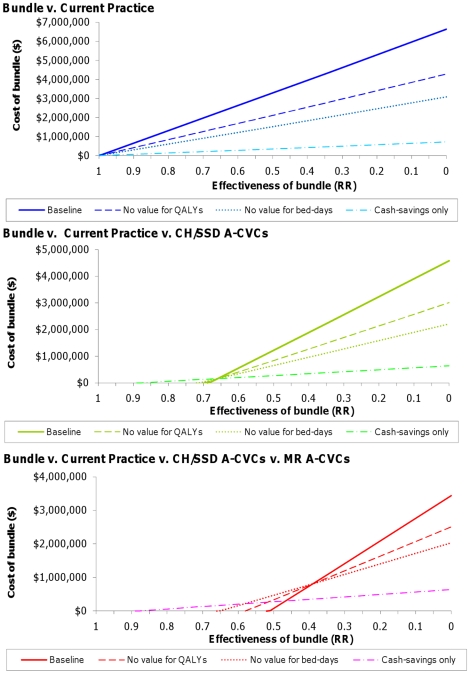
Methods and findings: A Markov decision model was used to evaluate the cost-effectiveness of the bundle relative to remaining with current practice (a non-bundled approach to catheter care and uncoated catheters), or use of antimicrobial catheters. We assumed the bundle reduced relative risk of CR-BSI to 0.34. Given uncertainty about the cost of the bundle, threshold analyses were used to determine the maximum cost at which the bundle remained cost-effective relative to the other approaches to infection control. Sensitivity analyses explored how this threshold alters under different assumptions about the economic value placed on bed-days and health benefits gained by preventing infection. If clinicians are prepared to use antimicrobial catheters, the bundle is cost-effective if national 18-month implementation costs are below $1.1 million. If antimicrobial catheters are not an option the bundle must cost less than $4.3 million. If decision makers are only interested in obtaining cash-savings for the unit, and place no economic value on either the bed-days or the health benefits gained through preventing infection, these cost thresholds are reduced by two-thirds.
Conclusions: A catheter care bundle has the potential to be cost-effective in the Australian intensive care setting. Rather than anticipating cash-savings from this intervention, decision makers must be prepared to invest resources in infection control to see efficiency improvements.
Conflict of interest statement
Figures
Similar articles
-
Cost effectiveness of antimicrobial catheters in the intensive care unit: addressing uncertainty in the decision.Crit Care. 2009;13(2):R35. doi: 10.1186/cc7744. Epub 2009 Mar 11. Crit Care. 2009. PMID: 19284570 Free PMC article.
-
Are educational interventions to prevent catheter-related bloodstream infections in intensive care unit cost-effective?J Hosp Infect. 2014 Jan;86(1):47-52. doi: 10.1016/j.jhin.2013.09.004. Epub 2013 Sep 21. J Hosp Infect. 2014. PMID: 24262140
-
[The effect of an intervention on rates of central vascular catheter-related bloodstream infection in intensive care units at the Hadassah Medical Center].Harefuah. 2013 Jan;152(1):16-20, 60. Harefuah. 2013. PMID: 23461020 Hebrew.
-
The clinical and economic consequences of nosocomial central venous catheter-related infection: are antimicrobial catheters useful?Infect Control Hosp Epidemiol. 2000 Jun;21(6):375-80. doi: 10.1086/501776. Infect Control Hosp Epidemiol. 2000. PMID: 10879567 Review.
-
Preventing catheter-related infections in cancer patients: a review of current strategies.Expert Rev Anti Infect Ther. 2020 Jun;18(6):531-538. doi: 10.1080/14787210.2020.1750367. Epub 2020 Apr 12. Expert Rev Anti Infect Ther. 2020. PMID: 32237923 Review.
Cited by
-
Indications and outcomes for tunneled central venous line placement via the axillary vein in children.Pediatr Surg Int. 2017 Sep;33(9):1001-1005. doi: 10.1007/s00383-017-4099-y. Epub 2017 Jun 27. Pediatr Surg Int. 2017. PMID: 28656388
-
Prevention of Central Line-Associated Bloodstream Infections Through Educational Interventions in Adult Intensive Care Units: A Systematic Review.Cureus. 2021 Aug 18;13(8):e17293. doi: 10.7759/cureus.17293. eCollection 2021 Aug. Cureus. 2021. PMID: 34552831 Free PMC article. Review.
-
epic3: national evidence-based guidelines for preventing healthcare-associated infections in NHS hospitals in England.J Hosp Infect. 2014 Jan;86 Suppl 1:S1-70. doi: 10.1016/S0195-6701(13)60012-2. J Hosp Infect. 2014. PMID: 24330862 Free PMC article.
-
Microbial diversity on intravascular catheters from paediatric patients.Eur J Clin Microbiol Infect Dis. 2015 Dec;34(12):2463-70. doi: 10.1007/s10096-015-2504-9. Epub 2015 Oct 29. Eur J Clin Microbiol Infect Dis. 2015. PMID: 26515578
-
Combining QOF data with the care bundle approach may provide a more meaningful measure of quality in general practice.BMC Health Serv Res. 2012 Oct 8;12:351. doi: 10.1186/1472-6963-12-351. BMC Health Serv Res. 2012. PMID: 23043262 Free PMC article.
References
-
- Blot SI, Depuydt P, Annemans L, Benoit D, Hoste E, et al. Clinical and economic outcomes in critically ill patients with nosocomial catheter-related bloodstream infections. Clinical Infectious Diseases. 2005;41:1591–1598. - PubMed
-
- Harbarth S, Sax H, Gastmeier P. The preventable proportion of nosocomial infections: an overview of published reports. Journal of Hospital Infection. 2003;54:258–266. - PubMed
-
- Berwick DM, Calkins DR, McCannon CJ, Hackbarth AD. The 100,000 Lives Campaign: Setting a goal and a deadline for improving health care quality. JAMA. 2006;295:324–327. - PubMed
-
- Centers for Medicare & Medicaid Services. Medicare Program: Changes to the hospital inpatient prospective payment systems and fiscal year 2009 rates; payments for graduate medical education in certain emergency situations; changes to disclosure of physician ownership in hospitals and physician self-referral rules; updates to the long-term care prospective payment system; updates to certain IPPS-excluded hospitals; and collection of information regarding financial relationships between hospitals; final rule. Federal Register. 2008;73:48434–49083. - PubMed
-
- Graves N, McGowan JE., Jr Nosocomial infection, the Deficit Reduction Act, and incentives for hospitals. JAMA. 2008;300:1577–1579. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
