

Surgical therapy of skeletal complications in multiple myeloma
- PMID: 20862584
- PMCID: PMC3167427
- DOI: 10.1007/s00264-010-1127-0
Surgical therapy of skeletal complications in multiple myeloma
Abstract
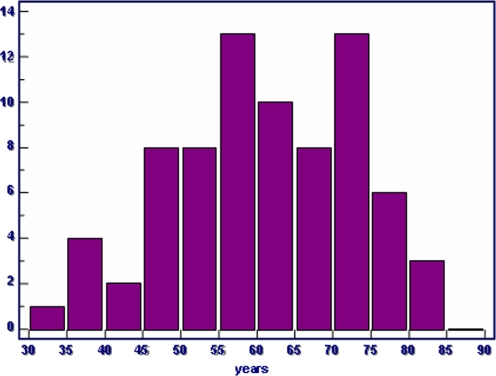
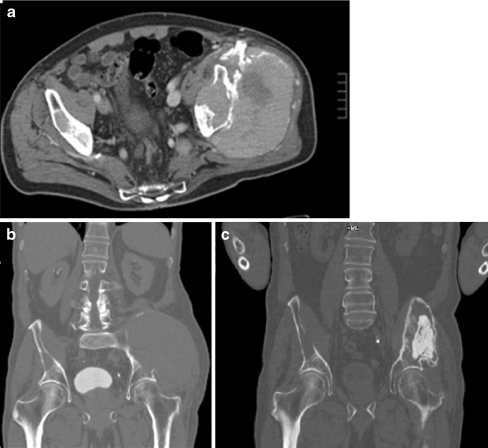
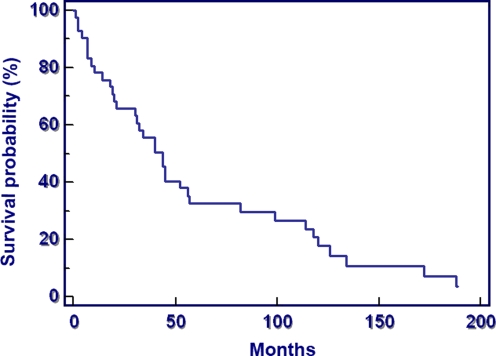
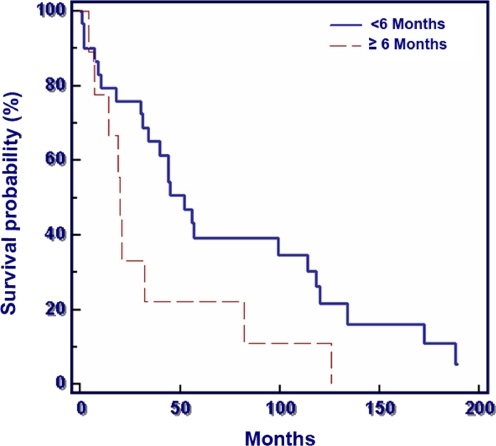
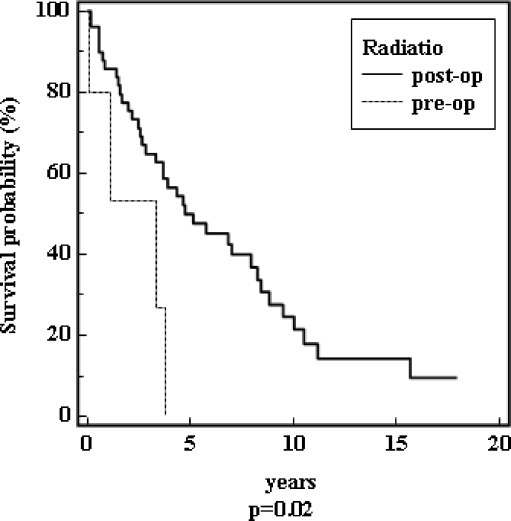
Patients with multiple myeloma are often treated surgically as though they have bone metastases. Due to major differences in oncological therapy and comparatively long survival times these patients should be considered separately. Seventy-five multiple myeloma patients were treated surgically (83 interventions) for skeletal complications of the disease. Location and dissemination, symptoms, method of surgery, complications, recurrence and survival time were evaluated retrospectively. Most of the lesions were in the axial skeleton or the proximal extremities apart from one distal lesion of the fibula, and most surgery was performed in the spine (35 patients). The mean follow-up of patients was 5.4 years (range 1-25 years). Survival proved to be very favourable (37% at five years). Patients with a single bone lesion, a negative bone marrow biopsy, no paraproteinaemia in serum or a Salmon-Durie-stage I had a better survival probability. Surgical treatment in patients with multiple myeloma was mostly limited to a palliative approach but survival time was better (37% at five years) than in patients with metastatic bone disease which has to be considered in their surgical treatment.
Figures
References
-
- Mundy GR, Bertolini DR. Bone destruction and hypercalcemia in plasma cell myeloma. Semin Oncol. 1986;13:291–299. - PubMed
-
- Kyle RA. Multiple myeloma: review of 869 cases. Mayo Clin Proc. 1975;50:29–40. - PubMed
-
- Chak LY, Cox RS, Bostwick DG, Hoppe RT. Solitary plasmacytoma of bone: treatment, progression, and survival. J Clin Oncol. 1987;5:1811–1815. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
