

Nighttime hospital blood pressure--a predictor of death, ESRD, and decline in GFR
- PMID: 20863206
- PMCID: PMC3146017
- DOI: 10.3109/0886022X.2010.510615
Nighttime hospital blood pressure--a predictor of death, ESRD, and decline in GFR
Abstract
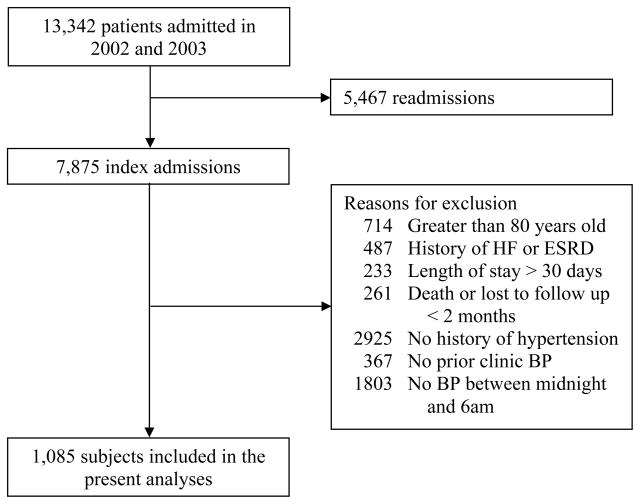
Nighttime systolic blood pressure (BP) from ambulatory blood pressure monitoring (ABPM) is more predictive than clinic BP for cardiovascular disease, stroke, and death even after controlling for clinic BP. However, ABPM is expensive and burdensome to obtain regularly. BPs obtained in the hospital may provide a window into nighttime BP. We conducted a retrospective cohort study of all hypertensive patients admitted to the Louis Stokes Cleveland Department of Veterans Affairs Medical Center (LSCDVAMC) in 2002 and 2003 with one or more BP recorded between midnight and 6 am on the day of or the day before discharge. The mean age of the study population (n = 1085) was 62 years and 96% were male. Twenty-two percent had coronary artery disease (CAD) and 34% had diabetes. The mean nighttime systolic BP was 132 mmHg and baseline glomerular filtration rate (GFR) was 83 mL/min per 1.73 m(2). Over a median follow-up period of 4.3 years, 266 subjects died, 22 developed end-stage renal disease (ESRD), 99 had a 50% decline in GFR, and 136 developed myocardial infarction (MI). The adjusted hazard ratios (HRs) associated with a 10 mmHg increase in nighttime systolic BP were 1.03 (95% confidence interval, 0.93-1.15) for death, 1.30 (0.94-1.80) for ESRD, 1.26 (1.08-1.47) for a 50% decline in GFR, 1.07 (0.92-1.23) for myocardial infarction, and 1.12 (1.03-1.23) for a composite of death, ESRD, or a 50% decline in GFR. In conclusion, nighttime systolic BP in hospitalized patients is an independent predictor of important clinical outcomes such as a composite of death, ESRD, or a 50% decline in GFR.
Conflict of interest statement
Figures
References
-
- Chobanian AV, Bakris GL, Black HR, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206–1252. - PubMed
-
- Padiyar A, Rahman M. Ambulatory blood pressure monitoring: an argument for wider clinical use. Cleve Clin J Med. 2007;74(11):831–838. - PubMed
-
- Fagard RH, Celis H, Thijs L, et al. Daytime and nighttime blood pressure as predictors of death and cause-specific cardiovascular events in hypertension. Hypertension. 2008;51(1):55–61. - PubMed
-
- Dolan E, Stanton A, Thijs L, et al. Superiority of ambulatory over clinic blood pressure measurement in predicting mortality: the Dublin outcome study. Hypertension. 2005;46(1):156–161. - PubMed
-
- Staessen JA, Thijs L, Fagard R, et al. Predicting cardiovascular risk using conventional vs ambulatory blood pressure in older patients with systolic hypertension. Systolic Hypertension in Europe Trial Investigators. JAMA. 1999;282(6):539–546. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous