

How many sonograms are needed to reliably predict the absence of fetal overgrowth in gestational diabetes mellitus pregnancies?
- PMID: 20864517
- PMCID: PMC3005443
- DOI: 10.2337/dc10-0415
How many sonograms are needed to reliably predict the absence of fetal overgrowth in gestational diabetes mellitus pregnancies?
Abstract
Objective: Serial measurements of the fetal abdominal circumference have been used to guide metabolic management of pregnancies complicated by gestational diabetes mellitus (GDM). A reduction in the number of repeat ultrasound examinations would save resources. Our purpose was to determine the number of serial abdominal circumference measurements per patient necessary to reliably predict the absence of fetal overgrowth.
Research design and methods: Women who had GDM were asked to return for repeat ultrasound at 3- to 4-week intervals starting at initiation of care (mean 26.9 ± 5.7 weeks). Maternal risk factors associated with fetal overgrowth were determined.
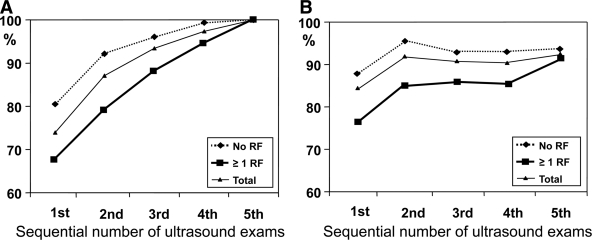
Results: A total of 4,478 ultrasound examinations were performed on 1,914 subjects (2.3 ± 1.2 per pregnancy). Of the 518 women with fetal abdominal circumference >90th percentile, it was diagnosed in 73.9% with the first ultrasound examination at entry and in 13.1% with the second ultrasound examination. Of the fetuses, 85.9 and 86.9% of the fetuses were born non-large for gestational age (LGA) when abdominal circumference was <90th percentile at 24-27 weeks and 28-32 weeks, respectively, and 88.0% were born non-LGA when both scans showed normal growth. For those women who had no risk factors for fetal overgrowth (risk factors: BMI >30 kg/m², history of macrosomia, and fasting glucose > 100 mg/dl), the accuracy of prediction of a non-LGA neonate was 90.0, 89.5, and 95.2%. The predictive ability did not increase with more than two normal scans.
Conclusions: The yield of sonographic diagnosis of a large fetus drops markedly after the finding of a fetal abdominal circumference <90th percentile on two sonograms, which excludes with high reliability the risk of a LGA newborn. The ability was enhanced in women who had no risk factors for neonatal macrosomia.
Figures
Similar articles
-
Determinants of fetal growth at different periods of pregnancies complicated by gestational diabetes mellitus or impaired glucose tolerance.Diabetes Care. 2003 Jan;26(1):193-8. doi: 10.2337/diacare.26.1.193. Diabetes Care. 2003. PMID: 12502680
-
Sonographic and other nonglycemic factors can predict large-for-gestational-age infants in diet-managed gestational diabetes mellitus: A retrospective cohort study.J Diabetes. 2020 Aug;12(8):562-572. doi: 10.1111/1753-0407.13042. Epub 2020 Apr 20. J Diabetes. 2020. PMID: 32250016
-
Large-for-gestational age diagnosed during second-trimester anatomy ultrasound and association with gestational diabetes and large-for-gestational age at birth.Ultrasound Obstet Gynecol. 2020 Dec;56(6):901-905. doi: 10.1002/uog.21930. Ultrasound Obstet Gynecol. 2020. PMID: 31763722
-
Ultrasound prediction of fetal macrosomia in pregnancies complicated by diabetes mellitus: a systematic review and meta-analysis.J Perinat Med. 2024 Jun 12;52(6):623-632. doi: 10.1515/jpm-2024-0121. Print 2024 Jul 26. J Perinat Med. 2024. PMID: 38860644
-
Additional single third trimester ultrasound scan in detection of large for gestational age fetuses.Curr Opin Obstet Gynecol. 2022 Oct 1;34(5):275-278. doi: 10.1097/GCO.0000000000000813. Epub 2022 Aug 24. Curr Opin Obstet Gynecol. 2022. PMID: 36036474 Review.
Cited by
-
High oleic/stearic fatty-acid desaturation index in cord plasma from infants of mothers with gestational diabetes.J Perinatol. 2014 May;34(5):357-63. doi: 10.1038/jp.2014.23. Epub 2014 Feb 27. J Perinatol. 2014. PMID: 24577432 Free PMC article.
-
ULTRASOUND DIAGNOSIS OF MACROSOMIA AMONG WOMEN WITH GESTATIONAL DIABETES - REVIEW OF THE LITERATURE.Acta Clin Croat. 2022 Mar;61(1):95-106. doi: 10.20471/acc.2022.61.01.12. Acta Clin Croat. 2022. PMID: 36398082 Free PMC article. Review.
-
[Gestational diabetes].Internist (Berl). 2011 Oct;52(10):1149-57. doi: 10.1007/s00108-011-2825-4. Internist (Berl). 2011. PMID: 21901407 Review. German.
-
Refining the diagnosis of gestational diabetes mellitus: a systematic review and meta-analysis.Commun Med (Lond). 2023 Dec 18;3(1):185. doi: 10.1038/s43856-023-00393-8. Commun Med (Lond). 2023. PMID: 38110524 Free PMC article.
-
A Clinical Update on Gestational Diabetes Mellitus.Endocr Rev. 2022 Sep 26;43(5):763-793. doi: 10.1210/endrev/bnac003. Endocr Rev. 2022. PMID: 35041752 Free PMC article.
References
-
- Metzger B, Buchanan T, Coustan D, De Leiva A, Dunger D, Hod M, Kitzmiller J, Kjos S, Oats J, Pettitt D, Sacks D, Zoupas C: Summary and recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007;30(Suppl.):S251–S260 - PubMed
-
- Sacks DA, Chen W: Estimating fetal weight in the management of macrosomia. Obstet Gynecol Surv 2000;55:229–239 - PubMed
-
- Jazayeri A, Heffron JA, Phillips R, Spellacy WN: Macrosomia prediction using ultrasound fetal abdominal circumference of 35 centimeters or more. Obstet Gynecol 1999;93:523–526 - PubMed
-
- De Reu PA, Smits LJ, Oosterbaan HP, Nijhuis JG: Value of a single early third trimester fetal biometry for the prediction of birth weight deviations in a low risk population. J Perinat Med 2008;36:324–329 - PubMed
-
- Bochner CJ, Medearis AL, Williams J, 3rd, Castro L, Hobel CJ, Wade ME: Early third-trimester ultrasound screening in gestational diabetes to determine the risk of macrosomia and labor dystocia at term. Am J Obstet Gynecol 1987;157:703–708 - PubMed
