

A diagnostic assay based on microRNA expression accurately identifies malignant pleural mesothelioma
- PMID: 20864637
- PMCID: PMC2963911
- DOI: 10.2353/jmoldx.2010.090169
A diagnostic assay based on microRNA expression accurately identifies malignant pleural mesothelioma
Abstract
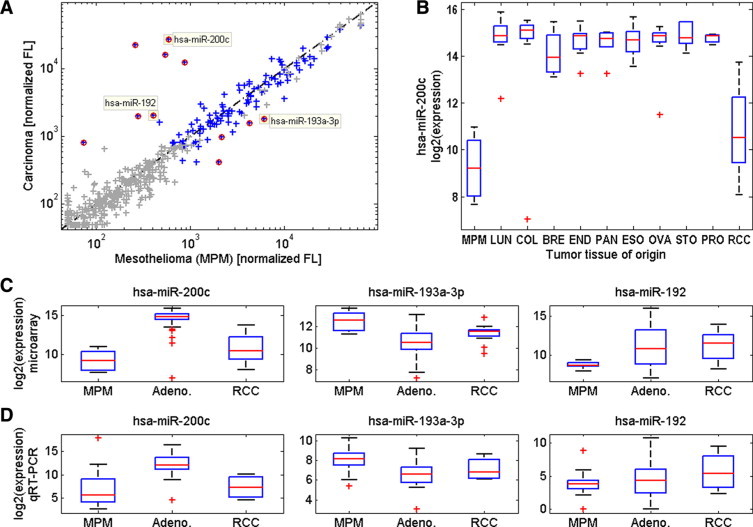
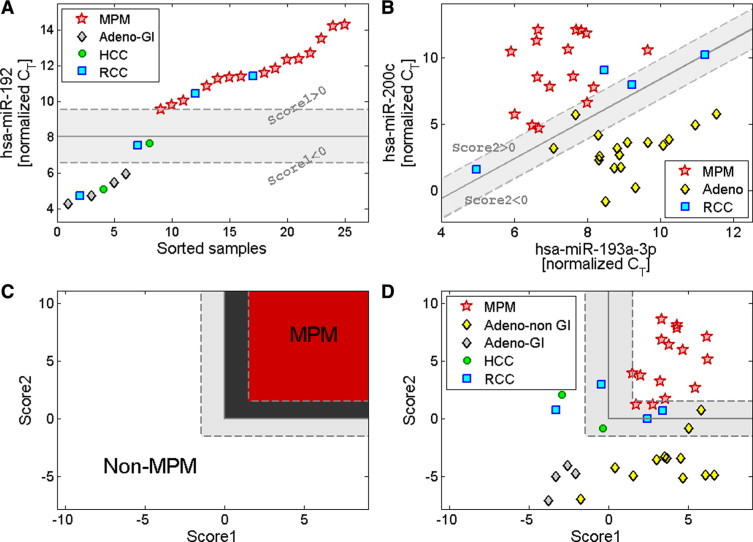
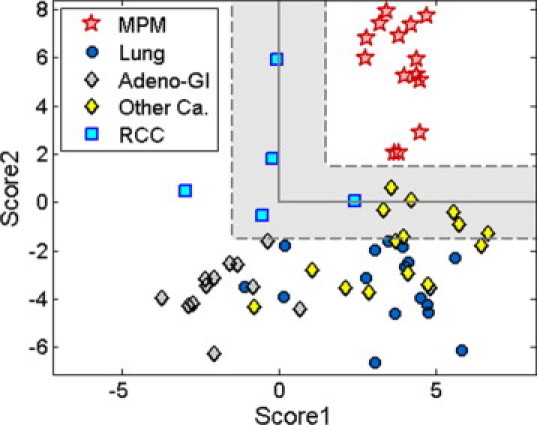
The definitive identification of malignant pleural mesothelioma (MPM) has significant clinical implications, yet other malignancies often involve the lung pleura, confounding the diagnosis of MPM. In the absence of accurate markers, MPM can be difficult to distinguish from peripheral lung adenocarcinoma and metastatic epithelial cancers. MicroRNA expression is tissue-specific and highly informative for identifying tumor origin. We identified microRNA biomarkers for the differential diagnosis of MPM and developed a standardized microRNA-based assay. Formalin-fixed, paraffin-embedded samples of 33 MPM and 210 carcinomas were used for assay development. Using microarrays, we identified microRNAs differentially expressed between MPM and various carcinomas. Hsa-miR-193-3p was overexpressed in MPM, while hsa-miR-200c and hsa-miR-192 were overexpressed in peripheral lung adenocarcinoma and carcinomas that frequently metastasize to lung pleura. We developed a standardized diagnostic assay based on the expression of these microRNAs. The assay reached a sensitivity of 100% and a specificity of 94% in a blinded validation set of 68 samples from the lung and pleura. This diagnostic assay can provide a useful tool in the differential diagnosis of MPM from other malignancies in the pleura.
Figures

References
-
- Zervos MD, Bizekis C, Pass HI. Malignant mesothelioma 2008. Curr Opin Pulm Med. 2008;14:303–309. - PubMed
-
- Ismail-Khan R, Robinson LA, Williams CC, Jr, Garrett CR, Bepler G, Simon GR. Malignant pleural mesothelioma: a comprehensive review. Cancer Control. 2006;13:255–263. - PubMed
-
- Yarborough CM. Chrysotile as a cause of mesothelioma: an assessment based on epidemiology. Crit Rev Toxicol. 2006;36:165–187. - PubMed
-
- Suzuki Y. Pathology of human malignant mesothelioma–preliminary analysis of 1,517 mesothelioma cases. Ind Health. 2001;39:183–185. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
