

Rapid implementation of an integrated large-scale HIV counseling and testing, malaria, and diarrhea prevention campaign in rural Kenya
- PMID: 20865049
- PMCID: PMC2928737
- DOI: 10.1371/journal.pone.0012435
Rapid implementation of an integrated large-scale HIV counseling and testing, malaria, and diarrhea prevention campaign in rural Kenya
Erratum in
- PLoS One. 2010;5(9). doi: 10.1371/annotation/cd255375-7cf9-4b56-a81f-ec57e360c472. Kahn, James [corrected to Khan, James G]
- PLoS One. 2011;6(6). doi:10.1371/annotation/b3e1590a-5814-4848-958e-2af40d318936. Khan, James G [corrected to Kahn, James G]
Abstract
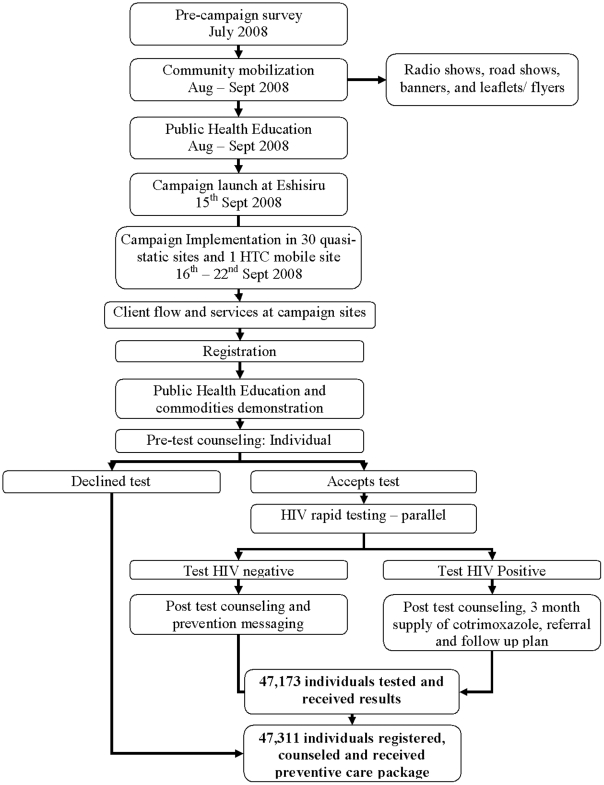
Background: Integrated disease prevention in low resource settings can increase coverage, equity and efficiency in controlling high burden infectious diseases. A public-private partnership with the Ministry of Health, CDC, Vestergaard Frandsen and CHF International implemented a one-week integrated multi-disease prevention campaign.
Method: Residents of Lurambi, Western Kenya were eligible for participation. The aim was to offer services to at least 80% of those aged 15-49. 31 temporary sites in strategically dispersed locations offered: HIV counseling and testing, 60 male condoms, an insecticide-treated bednet, a household water filter for women or an individual filter for men, and for those testing positive, a 3-month supply of cotrimoxazole and referral for follow-up care and treatment.
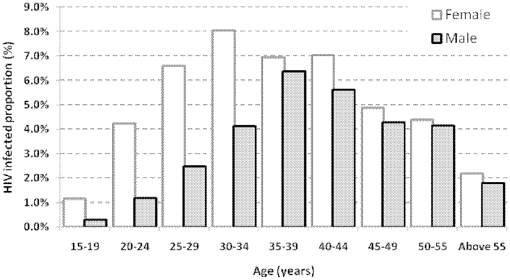
Findings: Over 7 days, 47,311 people attended the campaign with a 96% uptake of the multi-disease preventive package. Of these, 99.7% were tested for HIV (87% in the target 15-49 age group); 80% had previously never tested. 4% of those tested were positive, 61% were women (5% of women and 3% of men), 6% had median CD4 counts of 541 cell/µL (IQR; 356, 754). 386 certified counselors attended to an average 17 participants per day, consistent with recommended national figures for mass campaigns. Among women, HIV infection varied by age, and was more likely with an ended marriage (e.g. widowed vs. never married, OR.3.91; 95% CI. 2.87-5.34), and lack of occupation. In men, quantitatively stronger relationships were found (e.g. widowed vs. never married, OR.7.0; 95% CI. 3.5-13.9). Always using condoms with a non-steady partner was more common among HIV-infected women participants who knew their status compared to those who did not (OR.5.4 95% CI. 2.3-12.8).
Conclusion: Through integrated campaigns it is feasible to efficiently cover large proportions of eligible adults in rural underserved communities with multiple disease preventive services simultaneously achieving various national and international health development goals.
Conflict of interest statement
Figures
References
-
- World Health Organization, the Global Burden of Disease: 2004 update, published 2008. (accessed 2008) http://www.who.int/healthinfo/GBD_report_2004 update full.pdf.
-
- Centers for Disease Control and Prevention. CDC Activities in Kenya. (accessed 2010) http://www.cdc.gov/malaria/cdcactivities/kenya.htm.
-
- World Health Organization. EPIDEMIOLOGICAL PROFILE Population, endemicity and malaria burden. (accessed 2010) http://www.who.int.
-
- World Health Organization. Country profiles of Environmental Burden of Disease. (accessed 2010) http://www.who.int.
-
- Kenya AIDS Indicator Survey 2007, Preliminary Report. (accessed 2008.) http://www.aidskenya.org/
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
