

Interpreting meta-analysis according to the adequacy of sample size. An example using isoniazid chemoprophylaxis for tuberculosis in purified protein derivative negative HIV-infected individuals
- PMID: 20865104
- PMCID: PMC2943189
- DOI: 10.2147/clep.s9242
Interpreting meta-analysis according to the adequacy of sample size. An example using isoniazid chemoprophylaxis for tuberculosis in purified protein derivative negative HIV-infected individuals
Abstract
Objective: To illustrate the utility of statistical monitoring boundaries in meta-analysis, and provide a framework in which meta-analysis can be interpreted according to the adequacy of sample size. To propose a simple method for determining how many patients need to be randomized in a future trial before a meta-analysis can be deemed conclusive.
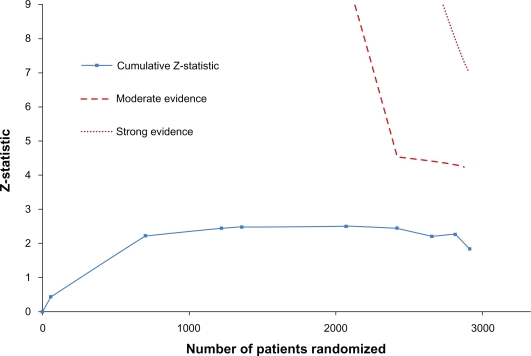
Study design and setting: Prospective meta-analysis of randomized clinical trials (RCTs) that evaluated the effectiveness of isoniazid chemoprophylaxis versus placebo for preventing the incidence of tuberculosis disease among human immunodeficiency virus (HIV)-positive individuals testing purified protein derivative negative. Assessment of meta-analysis precision using trial sequential analysis (TSA) with LanDeMets monitoring boundaries. Sample size determination for a future trials to make the meta-analysis conclusive according to the thresholds set by the monitoring boundaries.
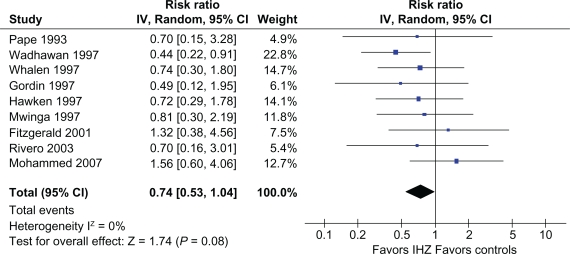
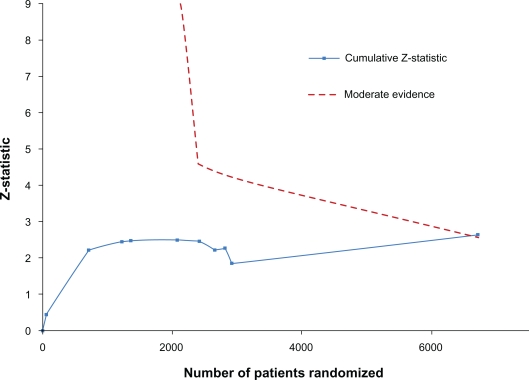
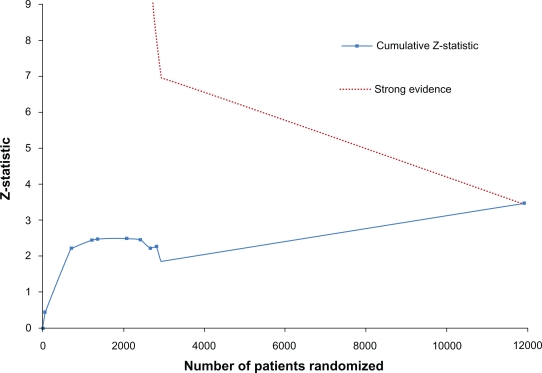
Results: The meta-analysis included nine trials comprising 2,911 trial participants and yielded a relative risk of 0.74 (95% CI, 0.53-1.04, P = 0.082, I(2) = 0%). To deem the meta-analysis conclusive according to the thresholds set by the monitoring boundaries, a future RCT would need to randomize 3,800 participants.
Conclusion: Statistical monitoring boundaries provide a framework for interpreting meta-analysis according to the adequacy of sample size and project the required sample size for a future RCT to make a meta-analysis conclusive.
Keywords: adequacy of sample size; human immunodeficiency virus (HIV); isoniazid chemoprophylaxis; meta-analysis; purified protein derivative negative; randomized clinical trials (RCTs); trial sequential analysis (TSA); tuberculosis.
Figures
References
-
- Guyatt G, Haynes RB, Jaeschke RZ, et al. Users’ Guides to the Medical Literature: XXV. Evidence-based medicine: principles for applying the Users’ Guides to patient care. JAMA. 2002;284:1290–1296. - PubMed
-
- Higgins JP, Green S. Cochrane Handbook for systematic reviews of interventions, version 5.0.0. Oxford: John Wiley & Sons; 2009.
-
- LeLorier J, Gregoire G, Benhaddad A, Lapierre J, Derderian F. Discrepancies between meta-analyses and subsequent large randomized, controlled trials. NEJM. 1997;337:536–542. - PubMed
-
- Moses LE, Mosteller F, Buehler JH. Comparing results of large clinical trials to those of meta-analysis. Stat Med. 2002;21:793–800. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
