

Current treatment options for recurrent nasopharyngeal cancer
- PMID: 20865269
- PMCID: PMC2966947
- DOI: 10.1007/s00405-010-1385-x
Current treatment options for recurrent nasopharyngeal cancer
Abstract
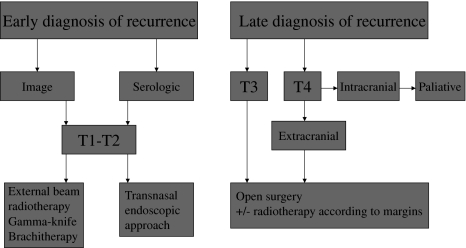
Loco-regional control rate of nasopharyngeal carcinoma (NPC) has improved significantly in the past decade. However, local recurrence still represents a major cause of mortality and morbidity in advanced stages, and management of local failure remains a challenging issue in NPC. The best salvage treatment for local recurrent NPC remains to be determined. The options include brachytherapy, external radiotherapy, stereotactic radiosurgery, and nasopharyngectomy, either alone or in different combinations. In this article we will discuss the different options for salvage of locally recurrent NPC. Retreatment of locally recurrent NPC using radiotherapy, alone or in combination with other treatment modalities, as well as surgery, can result in long-term local control and survival in a substantial proportion of patients. For small-volume recurrent tumors (T1-T2) treated with external radiotherapy, brachytherapy or stereotactic radiosurgery, comparable results to those obtained with surgery have been reported. In contrast, treatment results of advanced-stage locally recurrent NPC are generally more satisfactory with surgery (with or without postoperative radiotherapy) than with reirradiation.
Figures


References
-
- Lee AW, Law SC, Foo W, Poon YF, Cheung FK, Chan DK, Tung SY, Thaw M, Ho JH. Retrospective analysis of patients with nasopharyngeal carcinoma treated during 1976–1985: survival after local recurrence. Int J Radiat Oncol Biol Phys. 1993;26:773–782. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
