

Accuracy of SIAscopy for pigmented skin lesions encountered in primary care: development and validation of a new diagnostic algorithm
- PMID: 20868511
- PMCID: PMC2954906
- DOI: 10.1186/1471-5945-10-9
Accuracy of SIAscopy for pigmented skin lesions encountered in primary care: development and validation of a new diagnostic algorithm
Abstract
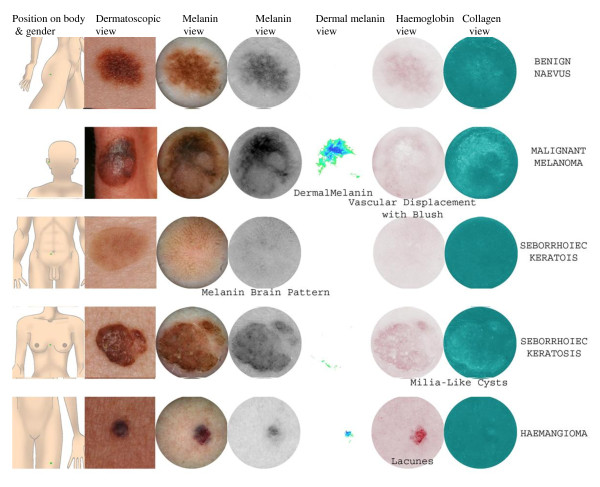
Background: Diagnosing pigmented skin lesions in general practice is challenging. SIAscopy has been shown to increase diagnostic accuracy for melanoma in referred populations. We aimed to develop and validate a scoring system for SIAscopic diagnosis of pigmented lesions in primary care.
Methods: This study was conducted in two consecutive settings in the UK and Australia, and occurred in three stages: 1) Development of the primary care scoring algorithm (PCSA) on a sub-set of lesions from the UK sample; 2) Validation of the PCSA on a different sub-set of lesions from the same UK sample; 3) Validation of the PCSA on a new set of lesions from an Australian primary care population. Patients presenting with a pigmented lesion were recruited from 6 general practices in the UK and 2 primary care skin cancer clinics in Australia. The following data were obtained for each lesion: clinical history; SIAscan; digital photograph; and digital dermoscopy. SIAscans were interpreted by an expert and validated against histopathology where possible, or expert clinical review of all available data for each lesion.
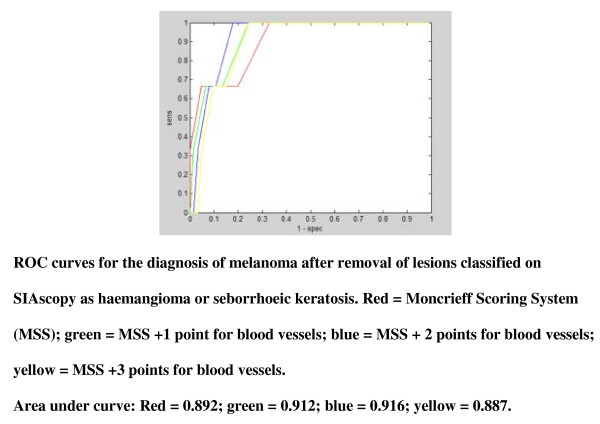
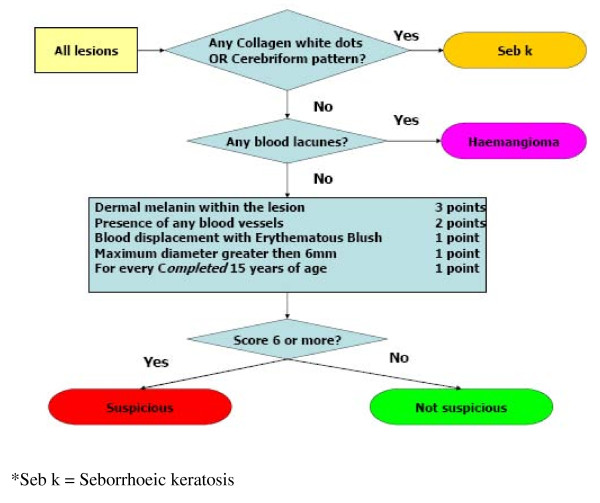
Results: A total of 858 patients with 1,211 lesions were recruited. Most lesions were benign naevi (64.8%) or seborrhoeic keratoses (22.1%); 1.2% were melanoma. The original SIAscopic diagnostic algorithm did not perform well because of the higher prevalence of seborrhoeic keratoses and haemangiomas seen in primary care. A primary care scoring algorithm (PCSA) was developed to account for this. In the UK sample the PCSA had the following characteristics for the diagnosis of 'suspicious': sensitivity 0.50 (0.18-0.81); specificity 0.84 (0.78-0.88); PPV 0.09 (0.03-0.22); NPV 0.98 (0.95-0.99). In the Australian sample the PCSA had the following characteristics for the diagnosis of 'suspicious': sensitivity 0.44 (0.32-0.58); specificity 0.95 (0.93-0.97); PPV 0.52 (0.38-0.66); NPV 0.95 (0.92-0.96). In an analysis of lesions for which histological diagnosis was available (n = 111), the PCSA had a significantly greater Area Under the Curve than the 7-point checklist for the diagnosis of melanoma (0.83; 95% CI 0.71-0.95 versus 0.61; 95% CI 0.44-0.78; p = 0.02 for difference).
Conclusions: The PCSA could have a useful role in improving primary care management of pigmented skin lesions. Further work is needed to develop and validate the PCSA in other primary care populations and to evaluate the cost-effectiveness of GP management of pigmented lesions using SIAscopy.
Figures

Similar articles
-
The cost-effectiveness of a novel SIAscopic diagnostic aid for the management of pigmented skin lesions in primary care: a decision-analytic model.Value Health. 2013 Mar-Apr;16(2):356-66. doi: 10.1016/j.jval.2012.12.008. Value Health. 2013. PMID: 23538188
-
Protocol for the MoleMate UK Trial: a randomised controlled trial of the MoleMate system in the management of pigmented skin lesions in primary care [ISRCTN 79932379].BMC Fam Pract. 2010 May 11;11:36. doi: 10.1186/1471-2296-11-36. BMC Fam Pract. 2010. PMID: 20459846 Free PMC article. Clinical Trial.
-
High-resolution ultrasound reflex transmission imaging and digital photography: potential tools for the quantitative assessment of pigmented lesions.Skin Res Technol. 2006 Feb;12(1):50-9. doi: 10.1111/j.0909-725X.2006.00136.x. Skin Res Technol. 2006. PMID: 16420539 Clinical Trial.
-
Role of In Vivo Reflectance Confocal Microscopy in the Analysis of Melanocytic Lesions.Acta Dermatovenerol Croat. 2018 Apr;26(1):64-67. Acta Dermatovenerol Croat. 2018. PMID: 29782304 Review.
-
Digital image analysis for diagnosis of cutaneous melanoma. Development of a highly effective computer algorithm based on analysis of 837 melanocytic lesions.Br J Dermatol. 2004 Nov;151(5):1029-38. doi: 10.1111/j.1365-2133.2004.06210.x. Br J Dermatol. 2004. PMID: 15541081 Review.
Cited by
-
A roadmap for the clinical implementation of optical-imaging biomarkers.Nat Biomed Eng. 2019 May;3(5):339-353. doi: 10.1038/s41551-019-0392-5. Epub 2019 Apr 29. Nat Biomed Eng. 2019. PMID: 31036890 Review.
-
Improving skin cancer detection by Raman spectroscopy using convolutional neural networks and data augmentation.Front Oncol. 2024 Jun 19;14:1320220. doi: 10.3389/fonc.2024.1320220. eCollection 2024. Front Oncol. 2024. PMID: 38962264 Free PMC article.
-
Current state of melanoma diagnosis and treatment.Cancer Biol Ther. 2019;20(11):1366-1379. doi: 10.1080/15384047.2019.1640032. Epub 2019 Aug 1. Cancer Biol Ther. 2019. PMID: 31366280 Free PMC article. Review.
-
Hyperspectral and multispectral image processing for gross-level tumor detection in skin lesions: a systematic review.J Biomed Opt. 2022 Jun;27(6):060901. doi: 10.1117/1.JBO.27.6.060901. J Biomed Opt. 2022. PMID: 35676751 Free PMC article.
-
Accessing Mole-Scanning through Community Pharmacy: A Pilot Service in Collaboration with Dermatology Specialists.Pharmacy (Basel). 2020 Dec 3;8(4):231. doi: 10.3390/pharmacy8040231. Pharmacy (Basel). 2020. PMID: 33287210 Free PMC article.
References
-
- UK skin cancer incidence statistics. CRUK. http://info.cancerresearchuk.org/cancerstats/types/skin/incidence
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
