

In vivo magnetic resonance imaging and optical imaging comparison of viable and nonviable mesenchymal stem cells with a bifunctional label
- PMID: 20868628
- PMCID: PMC3060764
In vivo magnetic resonance imaging and optical imaging comparison of viable and nonviable mesenchymal stem cells with a bifunctional label
Abstract
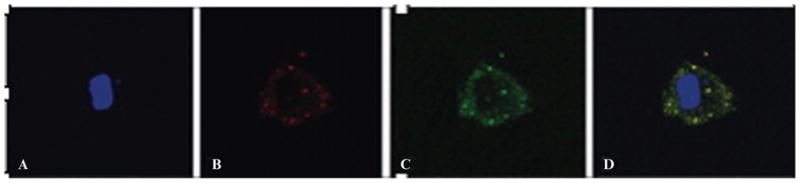
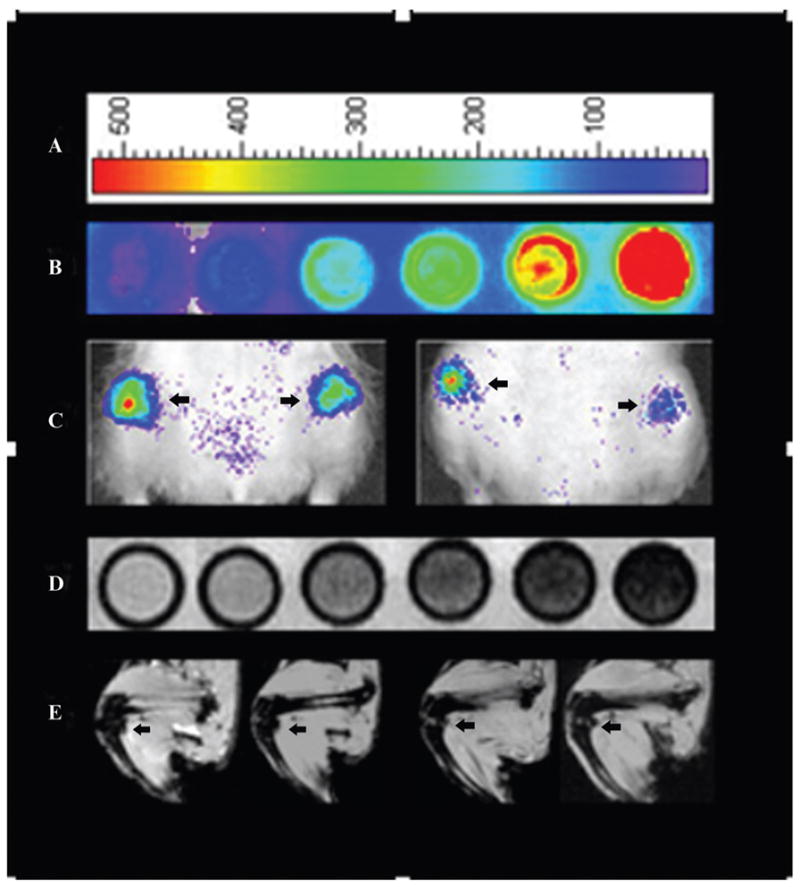
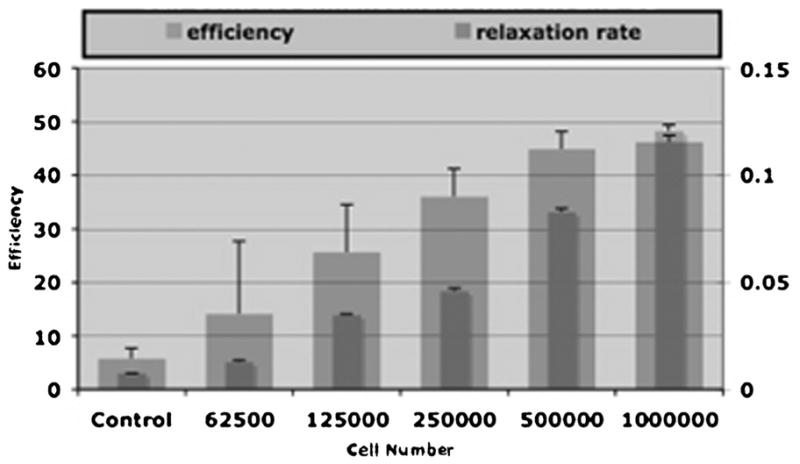
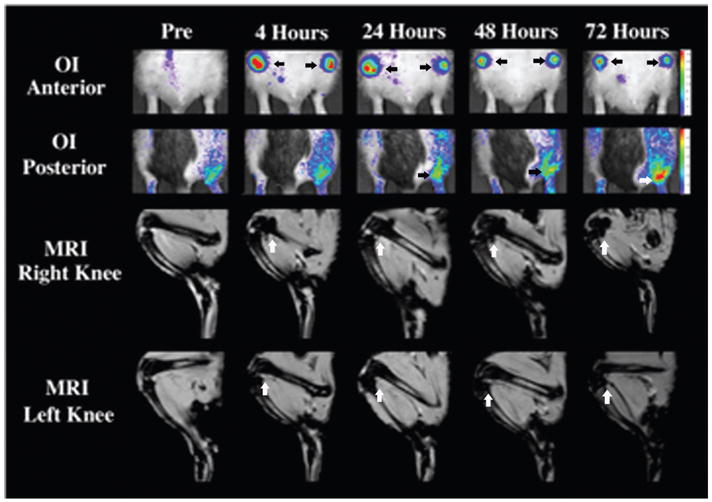
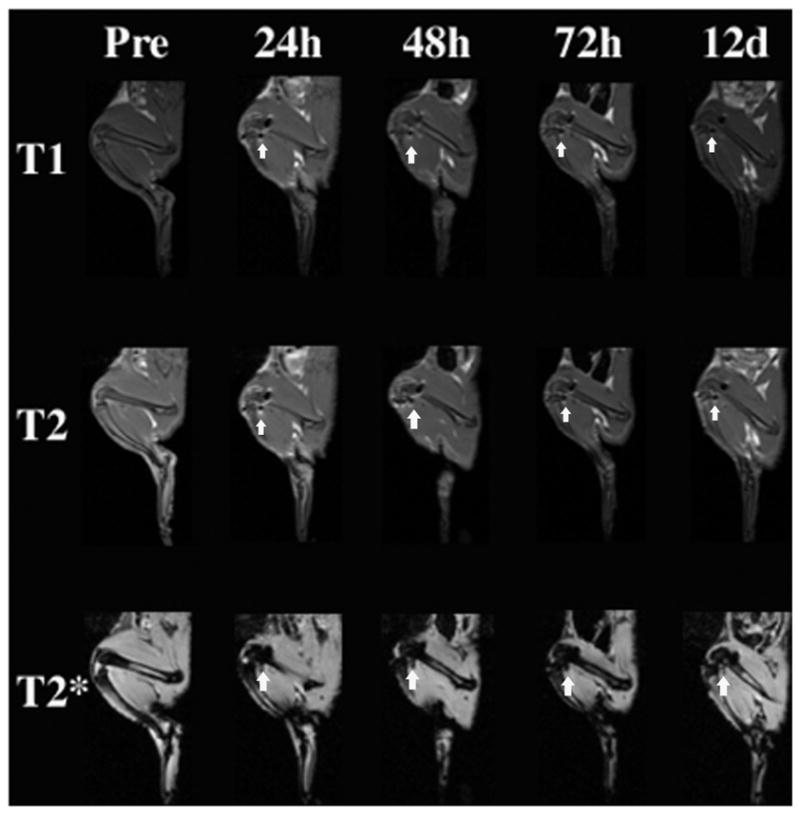
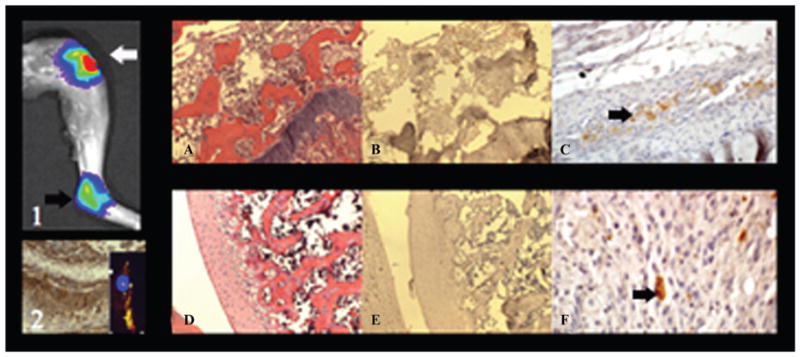
The purpose of this study was to compare viable and nonviable bilabeled mesenchymal stem cells (MSCs) in arthritic joints with magnetic resonance imaging (MRI) and optical imaging (OI). MSCs were labeled with ferucarbotran and DiD. MRI and OI of bilabeled cells were compared with controls. Six rats with arthritis received intra-articular injections of bilabeled viable MSCs into the right knee and nonviable MSCs into the left knee. Animals underwent MRI and OI preinjection and at 4, 24, 48, and 72 hours postinjection. The results were analyzed with a mixed random effects model and Fisher probability. Bilabeled MSCs showed increased MRI and OI signals compared to unlabeled controls (p < .0001). After intra-articular injection, bilabeled MSCs caused significant T2 and T2* effect on MRI and fluorescence on OI up to 72 hours postinjection (p < .05). There was no significant difference between viable and nonviable MSC signal in the knee joints; however, some of the viable cells migrated to an adjacent inflamed ankle joint (p < .05). Immunohistochemistry confirmed viable MSCs in right knee and ankle joints and nonviable MSCs in the left knee. Viable and nonviable cells could not be differentiated with MRI or OI signal intensity but were differentiated based on their ability to migrate in vivo.
Figures
References
-
- van Laar JM, Tyndall A. Adult stem cells in the treatment of autoimmune diseases. Rheumatology (Oxford) 2006;45:1187–93. - PubMed
-
- Djouad F, Fritz V, Apparailly F, et al. Reversal of the immunosuppressive properties of mesenchymal stem cells by tumor necrosis factor alpha in collagen-induced arthritis. Arthritis Rheum. 2005;52:1595–603. - PubMed
-
- Kostura L, Kraitchman DL, Mackay AM, et al. Feridex labeling of mesenchymal stem cells inhibits chondrogenesis but not adipogenesis or osteogenesis. NMR Biomed. 2004;17:513–7. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical