

Accuracy and quality of clinical decision rules for syncope in the emergency department: a systematic review and meta-analysis
- PMID: 20868906
- PMCID: PMC2946941
- DOI: 10.1016/j.annemergmed.2010.05.013
Accuracy and quality of clinical decision rules for syncope in the emergency department: a systematic review and meta-analysis
Abstract
Study objective: We assess the methodological quality and prognostic accuracy of clinical decision rules in emergency department (ED) syncope patients.
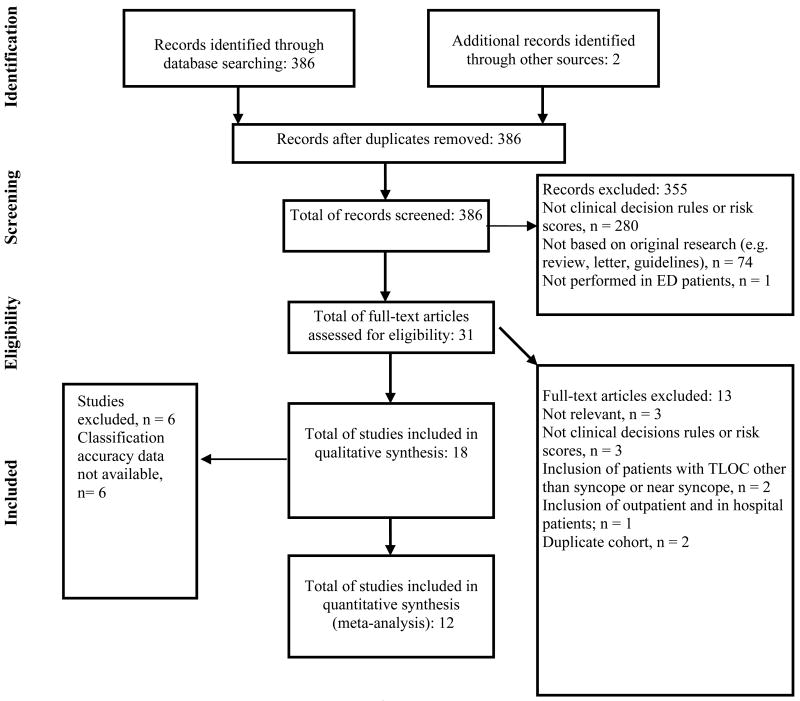
Methods: We searched 6 electronic databases, reviewed reference lists of included studies, and contacted content experts to identify articles for review. Studies that derived or validated clinical decision rules in ED syncope patients were included. Two reviewers independently screened records for relevance, selected studies for inclusion, assessed study quality, and abstracted data. Random-effects meta-analysis was used to pool diagnostic performance estimates across studies that derived or validated the same clinical decision rule. Between-study heterogeneity was assessed with the I(2) statistic, and subgroup hypotheses were tested with a test of interaction.
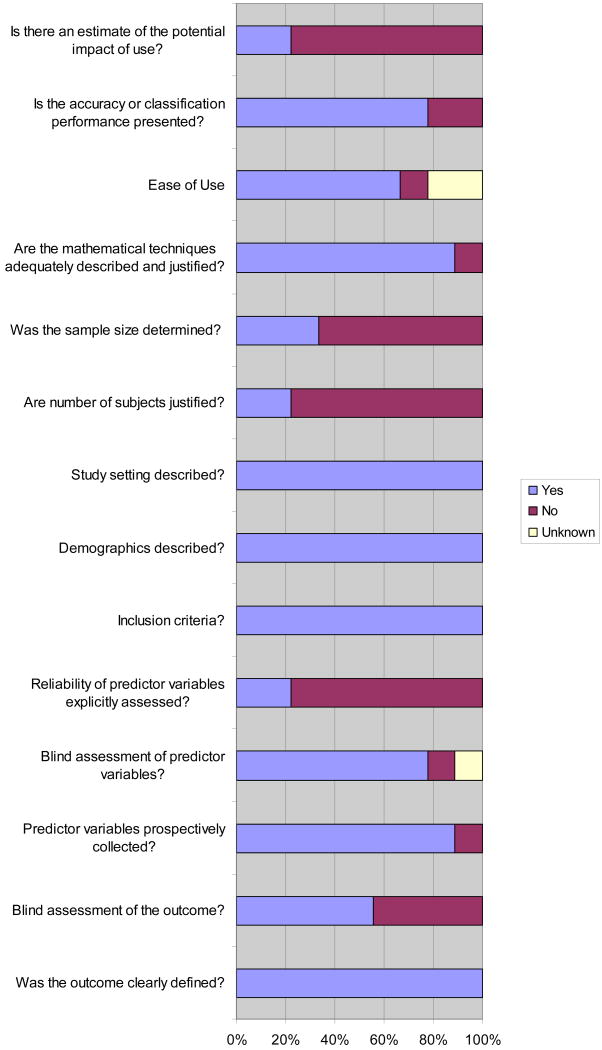
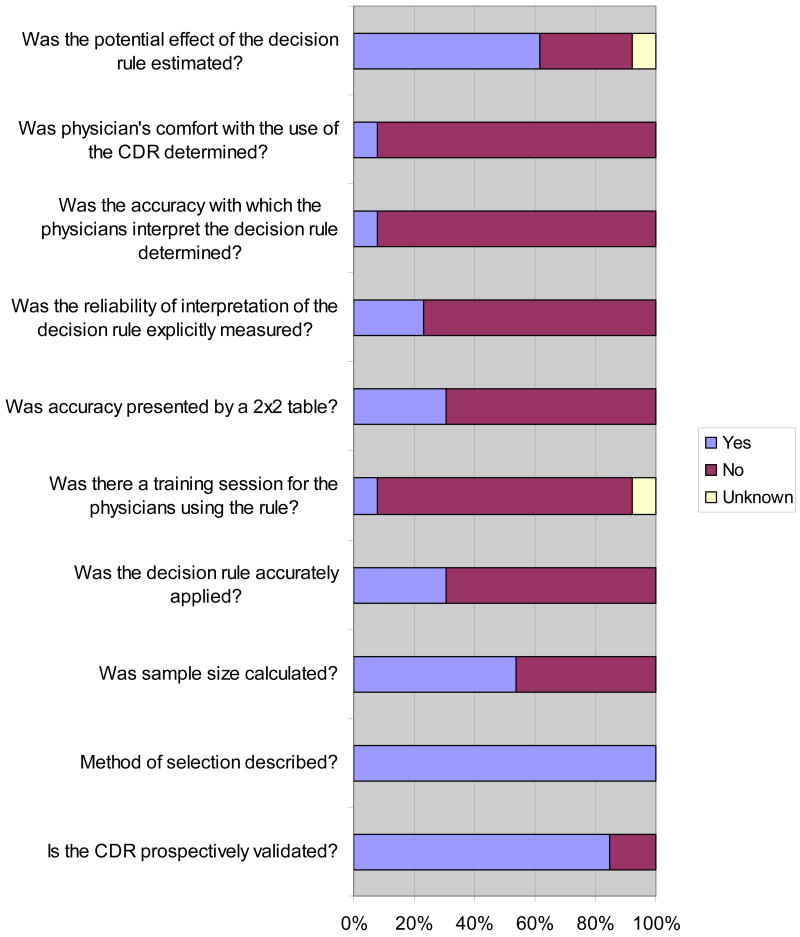
Results: We identified 18 eligible studies. Deficiencies in outcome (blinding) and interrater reliability assessment were the most common methodological weaknesses. Meta-analysis of the San Francisco Syncope Rule (sensitivity 86% [95% confidence interval {CI} 83% to 89%]; specificity 49% [95% CI 48% to 51%]) and the Osservatorio Epidemiologico sulla Sincope nel Lazio risk score (sensitivity 95% [95% CI 88% to 98%]; specificity 31% [95% CI 29% to 34%]). Subgroup analysis identified study design (prospective, diagnostic odds ratio 8.82 [95% CI 3.5 to 22] versus retrospective, diagnostic odds ratio 2.45 [95% CI 0.96 to 6.21]) and ECG determination (by evaluating physician, diagnostic odds ratio 25.5 [95% CI 4.41 to 148] versus researcher or cardiologist, diagnostic odds ratio 4 [95% CI 2.15 to 7.55]) as potential explanations for the variability in San Francisco Syncope Rule performance.
Conclusion: The methodological quality and prognostic accuracy of clinical decision rules for syncope are limited. Differences in study design and ECG interpretation may account for the variable prognostic performance of the San Francisco Syncope Rule when validated in different practice settings.
Copyright © 2010 American College of Emergency Physicians. Published by Mosby, Inc. All rights reserved.
Figures
References
-
- Huff JS, Decker WW, Quinn JV, et al. Clinical policy: critical issues in the evaluation and management of adult patients presenting to the emergency department with syncope. Journal of Emergency Nursing. 2007;33(6):e1–e17. - PubMed
-
- Alshekhlee A, Shen WK, Mackall J, et al. Incidence and mortality rates of syncope in the United States. The American journal of medicine. 2009 Feb;122(2):181–188. - PubMed
-
- Blanc JJ, L'Her C, Gosselin G, et al. Prospective evaluation of an educational programme for physicians involved in the management of syncope. Europace. 2005;7(4):400–406. - PubMed
-
- Quinn J, McDermott D, Stiell I, et al. Prospective validation of the San Francisco Syncope Rule to predict patients with serious outcomes. Ann Emerg Med. 2006 May;47(5):448–454. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
