

10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial
- PMID: 20870099
- PMCID: PMC2956884
- DOI: 10.1016/S0140-6736(10)61197-X
10-year stroke prevention after successful carotid endarterectomy for asymptomatic stenosis (ACST-1): a multicentre randomised trial
Abstract
Background: If carotid artery narrowing remains asymptomatic (ie, has caused no recent stroke or other neurological symptoms), successful carotid endarterectomy (CEA) reduces stroke incidence for some years. We assessed the long-term effects of successful CEA.
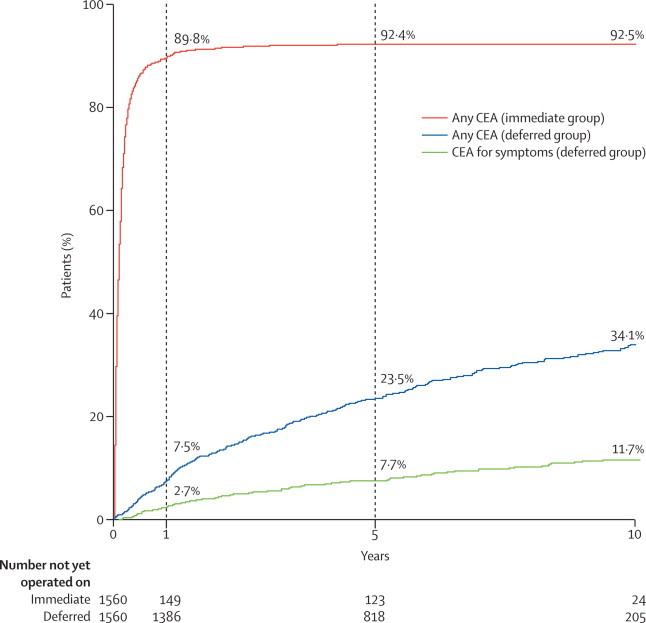
Methods: Between 1993 and 2003, 3120 asymptomatic patients from 126 centres in 30 countries were allocated equally, by blinded minimised randomisation, to immediate CEA (median delay 1 month, IQR 0·3-2·5) or to indefinite deferral of any carotid procedure, and were followed up until death or for a median among survivors of 9 years (IQR 6-11). The primary outcomes were perioperative mortality and morbidity (death or stroke within 30 days) and non-perioperative stroke. Kaplan-Meier percentages and logrank p values are from intention-to-treat analyses. This study is registered, number ISRCTN26156392.
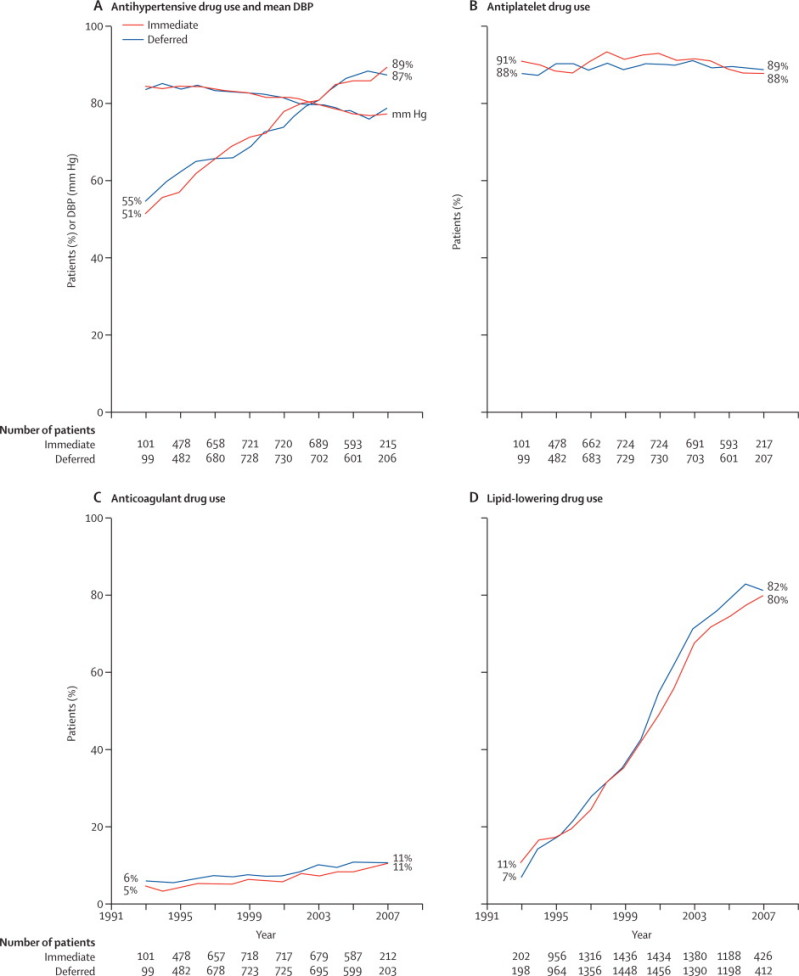
Findings: 1560 patients were allocated immediate CEA versus 1560 allocated deferral of any carotid procedure. The proportions operated on while still asymptomatic were 89·7% versus 4·8% at 1 year (and 92·1%vs 16·5% at 5 years). Perioperative risk of stroke or death within 30 days was 3·0% (95% CI 2·4-3·9; 26 non-disabling strokes plus 34 disabling or fatal perioperative events in 1979 CEAs). Excluding perioperative events and non-stroke mortality, stroke risks (immediate vs deferred CEA) were 4·1% versus 10·0% at 5 years (gain 5·9%, 95% CI 4·0-7·8) and 10·8% versus 16·9% at 10 years (gain 6·1%, 2·7-9·4); ratio of stroke incidence rates 0·54, 95% CI 0·43-0·68, p<0·0001. 62 versus 104 had a disabling or fatal stroke, and 37 versus 84 others had a non-disabling stroke. Combining perioperative events and strokes, net risks were 6·9% versus 10·9% at 5 years (gain 4·1%, 2·0-6·2) and 13·4% versus 17·9% at 10 years (gain 4·6%, 1·2-7·9). Medication was similar in both groups; throughout the study, most were on antithrombotic and antihypertensive therapy. Net benefits were significant both for those on lipid-lowering therapy and for those not, and both for men and for women up to 75 years of age at entry (although not for older patients).
Interpretation: Successful CEA for asymptomatic patients younger than 75 years of age reduces 10-year stroke risks. Half this reduction is in disabling or fatal strokes. Net benefit in future patients will depend on their risks from unoperated carotid lesions (which will be reduced by medication), on future surgical risks (which might differ from those in trials), and on whether life expectancy exceeds 10 years.
Funding: UK Medical Research Council, BUPA Foundation, Stroke Association.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures




Comment in
-
Lessons from carotid endarterectomy and stenting trials.Lancet. 2010 Sep 25;376(9746):1028-31. doi: 10.1016/S0140-6736(10)61415-8. Lancet. 2010. PMID: 20870079 No abstract available.
-
Best medical treatment for a symptomatic carotid artery stenosis.Lancet. 2011 Jan 8;377(9760):123; author reply 123-4. doi: 10.1016/S0140-6736(11)60015-9. Lancet. 2011. PMID: 21215879 No abstract available.
-
ACP Journal Club. Immediate surgery reduced long-term risk for nonperioperative stroke in severe asymptomatic carotid artery stenosis.Ann Intern Med. 2011 Feb 15;154(4):JC2-7. doi: 10.7326/0003-4819-154-4-201102150-02007. Ann Intern Med. 2011. PMID: 21320934 No abstract available.
References
-
- MRC Asymptomatic Carotid Surgery Trial (ACST) Collaborative Group Prevention of disabling and fatal strokes by successful carotid endarterectomy in patients without recent neurological symptoms: randomised controlled trial. Lancet. 2004;363:1491–1502. - PubMed
-
- Executive Committee for the Asymptomatic Carotid Artery Study Endarterectomy for asymptomatic carotid stenosis. JAMA. 1995;273:1421–1428. - PubMed
-
- Rothwell PM, Eliasziw M, Gutnikov SA, for the Carotid Endartectomy Trialists' Collaboration Analysis of pooled data from the randomised controlled trials of endarterectomy for symptomatic carotid stenosis. Lancet. 2003;361:107–116. - PubMed
-
- Baigent C, Peto R, Gray R, Parish S, Collins R. Large-scale randomized evidence: trials and meta-analyses of trials. In: Warrell DA, Firth JD, editors. Oxford Textbook of Medicine. 5th edn. Oxford University Press; Oxford: 2010. pp. 31–45.
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
