

Individualized strategy for dosing luteinizing hormone-releasing hormone agonists for androgen-independent prostate cancer: identification of outcomes and costs
- PMID: 20871718
- PMCID: PMC2794621
- DOI: 10.1200/JOP.2006.2.2.57
Individualized strategy for dosing luteinizing hormone-releasing hormone agonists for androgen-independent prostate cancer: identification of outcomes and costs
Abstract
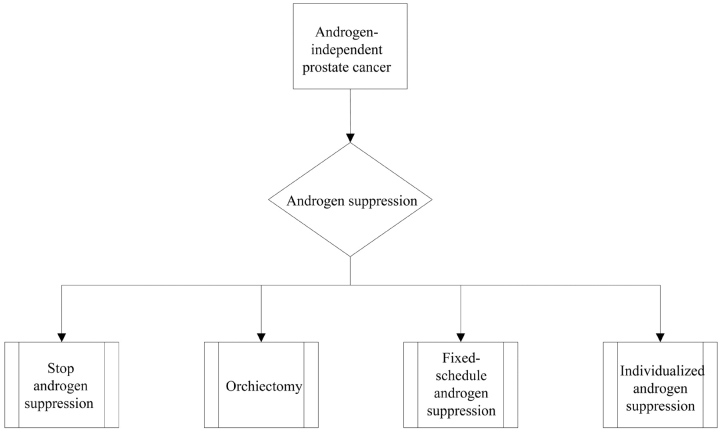
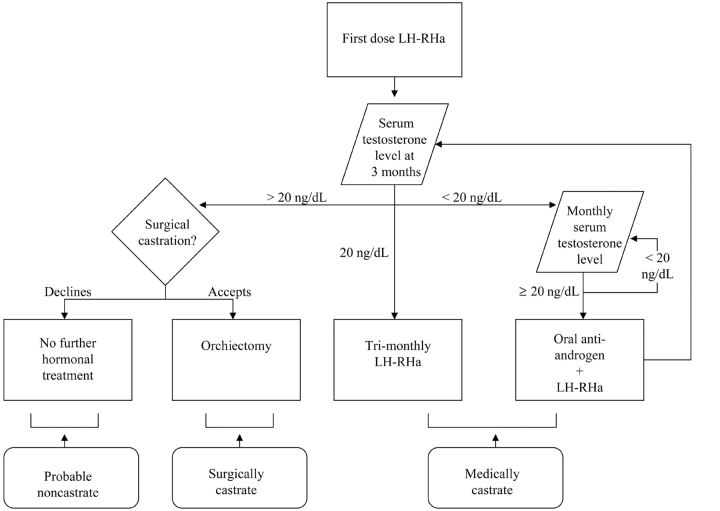
Purpose: Continuing androgen suppression is the current standard in men with androgen-independent prostate cancer (AIPC). An individualized strategy, wherein luteinizing hormone-releasing hormone agonists (LH-RHas) are redosed when serum testosterone approaches a non-castrate level, may decrease costs without worsening outcomes. To understand possible outcomes, we performed a cost-utility analysis comparing individualized and fixed LH-RHa dosing strategies in men with AIPC.
Methods: The model used a societal perspective, a 5-year time horizon, and 3% annual cost discounting. The model accounted for direct costs of androgen suppression. Utilities were varied in accordance with published preference data.
Results: Under base-case assumptions, individualized LH-RHa dosing yielded 1.089 expected quality-adjusted life years (QALYs), compared with 1.094 expected QALYs for fixed LH-RHa dosing. In cost analysis, lifetime per-patient costs for androgen suppression were estimated to be $5,694 for individualized LH-RHa dosing and $9,157 for fixed LH-RHa dosing. Applied to the total population, a strategy of individualized LH-RHa dosing would cost $170 million for androgen suppression, compared with $274 million for fixed LH-RHa dosing. Under these assumptions, adopting the individualized strategy resulted in $692,600 gained from a societal perspective for each QALY lost (the decremental cost utility).
Conclusion: The results suggest that an individualized LH-RHa dosing strategy would be associated with moderate savings on an individual basis but substantial savings on a population basis, and would not adversely affect quality of life or life expectancy. Further research is needed to establish the effects of this strategy on symptoms and survival, as well as patient satisfaction and true costs.
Figures
Similar articles
-
The cost-effectiveness of combined androgen blockade with bicalutamide and luteinizing hormone releasing hormone agonist in men with metastatic prostate cancer.J Urol. 2005 Aug;174(2):547-52; discussion 552. doi: 10.1097/01.ju.0000165569.48372.4c. J Urol. 2005. PMID: 16006889
-
Cost-effectiveness of androgen suppression therapies in advanced prostate cancer.J Natl Cancer Inst. 2000 Nov 1;92(21):1731-9. doi: 10.1093/jnci/92.21.1731. J Natl Cancer Inst. 2000. PMID: 11058616
-
Determining dosing intervals for luteinizing hormone releasing hormone agonists based on serum testosterone levels: a prospective study.J Urol. 2007 Jun;177(6):2132-5; discussion 2135. doi: 10.1016/j.juro.2007.01.157. J Urol. 2007. PMID: 17509298 Clinical Trial.
-
Luteinising hormone releasing hormone agonists (LH-RHa) in premenopausal early breast cancer patients: current role and future perspectives.Cancer Treat Rev. 2011 May;37(3):208-11. doi: 10.1016/j.ctrv.2010.07.007. Epub 2010 Aug 17. Cancer Treat Rev. 2011. PMID: 20724078 Review.
-
[Clinical evaluation of hot flushes developing during endocrine therapy for prostate carcinoma].Nihon Hinyokika Gakkai Zasshi. 2003 Sep;94(6):614-20. doi: 10.5980/jpnjurol1989.94.614. Nihon Hinyokika Gakkai Zasshi. 2003. PMID: 14531271 Review. Japanese.
Cited by
-
Cost savings and luteinizing hormone-releasing hormone agonist.J Oncol Pract. 2006 May;2(3):103. doi: 10.1200/JOP.2006.2.3.103. J Oncol Pract. 2006. PMID: 20871707 Free PMC article. No abstract available.
-
Kinetics of serum androgen normalization and factors associated with testosterone reserve after limited androgen deprivation therapy for nonmetastatic prostate cancer.J Urol. 2008 Oct;180(4):1432-7; discussion 1437. doi: 10.1016/j.juro.2008.06.017. Epub 2008 Aug 16. J Urol. 2008. PMID: 18710748 Free PMC article. Clinical Trial.
-
Even more cost savings?J Oncol Pract. 2006 Jul;2(4):202. doi: 10.1200/JOP.2006.2.4.202. J Oncol Pract. 2006. PMID: 20859336 Free PMC article. No abstract available.
-
Decrementally cost-effective health technologies in non-inferiority studies: A systematic review.Front Pharmacol. 2022 Dec 5;13:1025326. doi: 10.3389/fphar.2022.1025326. eCollection 2022. Front Pharmacol. 2022. PMID: 36545305 Free PMC article.
References
-
- American Cancer Society. Cancer Facts & Figures. 2004. http://www.cancer.org/downloads/STT/CAFF_finalPWSecured.pdf.
-
- Piper NY, Kusada L, Lance R, et al. Adenocarcinoma of the prostate: An expensive way to die. Prostate Cancer Prostatic Dis. 2002;5:164–166. - PubMed
-
- Taylor CD, Elson P, Trump DL. Importance of continued testicular suppression in hormone-refractory prostate cancer. J Clin Oncol. 1993;11:2167–2172. - PubMed
-
- Chon JK, Jacobs SC, Naslund MJ. The cost value of medical versus surgical hormonal therapy for metastatic prostate cancer. J Urol. 2000;64:735–737. - PubMed
-
- Hillner BE, Roberts JD. Role of perspective and other uncertainties in cost-effectiveness assessments in advanced prostate cancer. J Natl Cancer Inst. 2000;92:1704–1706. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
