

What Limits Cardiac Performance during Exercise in Normal Subjects and in Healthy Fontan Patients?
- PMID: 20871839
- PMCID: PMC2943078
- DOI: 10.1155/2010/791291
What Limits Cardiac Performance during Exercise in Normal Subjects and in Healthy Fontan Patients?
Abstract
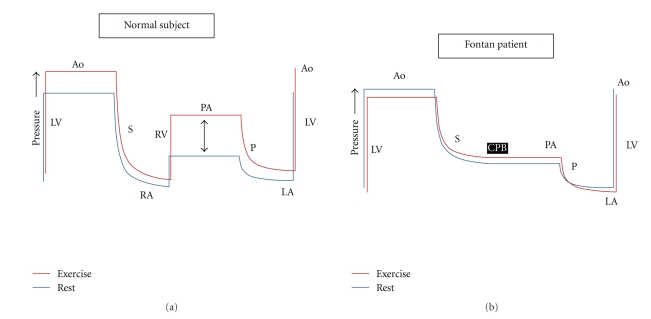
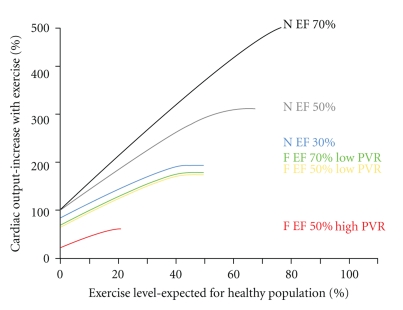
Exercise is an important determinant of health but is significantly reduced in the patient with a univentricular circulation. Normal exercise physiology mandates an increase in pulmonary artery pressures which places an increased work demand on the right ventricle (RV). In a biventricular circulation with pathological increases in pulmonary vascular resistance and/or reductions in RV function, exercise-induced augmentation of cardiac output is limited. Left ventricular preload reserve is dependent upon flow through the pulmonary circulation and this requires adequate RV performance. In the Fontan patient, the reasons for exercise intolerance are complex. In those patients with myocardial dysfunction or other pathologies of the circulatory components, it is likely that these abnormalities serve as a limitation to cardiac performance during exercise. However, in the healthy Fontan patient, it may be the absence of a sub-pulmonary pump which limits normal increases in pulmonary pressures, trans-pulmonary flow requirements and cardiac output. If so, performance will be exquisitely dependent on pulmonary vascular resistance. This provides a potential explanation as to why pulmonary vasodilators may improve exercise tolerance. As has recently been demonstrated, these agents may offer an important new treatment strategy which directly addresses the physiological limitations in the Fontan patient.
Figures
Similar articles
-
Pulmonary vascular disease in Fontan circulation-is there a rationale for pulmonary vasodilator therapies?Cardiovasc Diagn Ther. 2021 Aug;11(4):1111-1121. doi: 10.21037/cdt-20-431. Cardiovasc Diagn Ther. 2021. PMID: 34527537 Free PMC article. Review.
-
The pulmonary vascular bed in patients with functionally univentricular physiology and a Fontan circulation.Cardiol Young. 2021 Aug;31(8):1241-1250. doi: 10.1017/S104795112100192X. Epub 2021 Aug 11. Cardiol Young. 2021. PMID: 34378498 Review.
-
Heart Rate Reserve in Fontan Patients: Chronotropic Incompetence or Hemodynamic Limitation?J Am Heart Assoc. 2019 May 7;8(9):e012008. doi: 10.1161/JAHA.119.012008. J Am Heart Assoc. 2019. PMID: 31041880 Free PMC article.
-
Ventricular afterload and ventricular work in fontan circulation: comparison with normal two-ventricle circulation and single-ventricle circulation with blalock-taussig shunts.Circulation. 2002 Jun 18;105(24):2885-92. doi: 10.1161/01.cir.0000018621.96210.72. Circulation. 2002. Retraction in: Circulation. 2012 Jun 12;125(23):e1020. doi: 10.1161/CIR.0b013e31825f6499. PMID: 12070118 Retracted. Clinical Trial.
-
Cavopulmonary assist: circulatory support for the univentricular Fontan circulation.Ann Thorac Surg. 2003 Dec;76(6):1911-6; discussion 1916. doi: 10.1016/s0003-4975(03)01014-2. Ann Thorac Surg. 2003. PMID: 14667610
Cited by
-
The Fontan circulation after 45 years: update in physiology.Heart. 2016 Jul 15;102(14):1081-6. doi: 10.1136/heartjnl-2015-307467. Epub 2016 May 24. Heart. 2016. PMID: 27220691 Free PMC article. Review.
-
Inhaled iloprost for the treatment of patient with Fontan circulation.Korean J Pediatr. 2014 Oct;57(10):461-3. doi: 10.3345/kjp.2014.57.10.461. Epub 2014 Oct 31. Korean J Pediatr. 2014. PMID: 25379048 Free PMC article.
-
Cardiovascular Imaging-Derived Skeletal Muscle Mass Correlates With Fitness and Survival in Patients With Univentricular Circulation.Cureus. 2024 Mar 16;16(3):e56276. doi: 10.7759/cureus.56276. eCollection 2024 Mar. Cureus. 2024. PMID: 38623109 Free PMC article.
-
Decision-Making for Surgery in the Management of Patients with Univentricular Heart.Front Pediatr. 2015 Jul 27;3:61. doi: 10.3389/fped.2015.00061. eCollection 2015. Front Pediatr. 2015. PMID: 26284226 Free PMC article. Review.
-
Orthostatic stress response in pediatric Fontan patients and the effect of ACE inhibition.PLoS One. 2022 Sep 1;17(9):e0273940. doi: 10.1371/journal.pone.0273940. eCollection 2022. PLoS One. 2022. PMID: 36048833 Free PMC article.
References
-
- La Gerche A, Prior DL. Exercise: is it possible to have too much of a good thing? Heart Lung and Circulation. 2007;16(supplement 3):S102–S104. - PubMed
-
- Rowland T. Echocardiography and circulatory response to progressive endurance exercise. Sports Medicine. 2008;38(7):541–551. - PubMed
-
- La Gerche André, Macisaac AndrewI, Burns AndrewT, et al. Pulmonary transit of agitated contrast is associated with enhanced pulmonary vascular reserve and right ventricular function during exercise. Journal of Applied Physiology. In press. - PubMed
-
- Stanek V, Jebavy P, Hurych J, Widimsky J. Central haemodynamics during supine exercise and pulmonary artery occlusion in normal subjects. Bulletin de Physio-Pathologie Respiratoire. 1973;9(5):1203–1217. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
