

A cluster-randomized trial of a primary care informatics-based system for breast cancer screening
- PMID: 20872083
- PMCID: PMC3019316
- DOI: 10.1007/s11606-010-1500-0
A cluster-randomized trial of a primary care informatics-based system for breast cancer screening
Abstract
Background: Information technology offers the promise, as yet unfulfilled, of delivering efficient, evidence-based health care.
Objective: To evaluate whether a primary care network-based informatics intervention can improve breast cancer screening rates.
Design: Cluster-randomized controlled trial of 12 primary care practices conducted from March 20, 2007 to March 19, 2008.
Patients: Women 42-69 years old with no record of a mammogram in the prior 2 years.
Interventions: In intervention practices, a population-based informatics system was implemented that: connected overdue patients to appropriate care providers, presented providers with a Web-based list of their overdue patients in a non-visit-based setting, and enabled "one-click" mammography ordering or documented deferral reasons. Patients selected for mammography received automatically generated letters and follow-up phone calls. All practices had electronic health record reminders about breast cancer screening available during clinical encounters.
Main measures: The primary outcome was the proportion of overdue women undergoing mammography at 1-year follow-up.
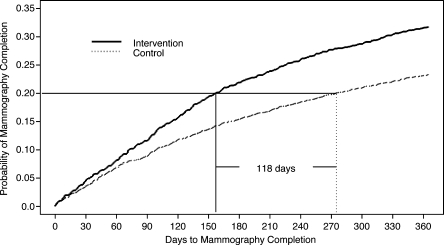
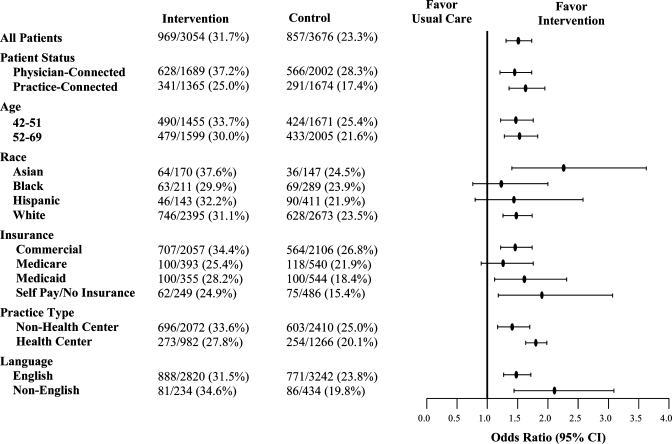
Key results: Baseline mammography rates in intervention and control practices did not differ (79.5% vs 79.3%, p = 0.73). Among 3,054 women in intervention practices and 3,676 women in control practices overdue for mammograms, intervention patients were somewhat younger, more likely to be non-Hispanic white, and have health insurance. Most intervention providers used the system (65 of 70 providers, 92.9%). Action was taken for 2,652 (86.8%) intervention patients [2,274 (74.5%) contacted and 378 (12.4%) deferred]. After 1 year, mammography rates were significantly higher in the intervention arm (31.4% vs 23.3% in control arm, p < 0.001 after adjustment for baseline differences; 8.1% absolute difference, 95% CI 5.1-11.2%). All demographic subgroups benefited from the intervention. Intervention patients completed screening sooner than control patients (p < 0.001).
Conclusions: A novel population-based informatics system functioning as part of a non-visit-based care model increased mammography screening rates in intervention practices.
Trial registration: ClinicalTrials.gov; NCT00462891.
Figures

References
-
- Armstrong K, Moye E, Williams S, et al. Screening mammography in women 40 to 49 years of age: a systematic review for the American College of Physicians. Ann Intern Med. 2007;146(7):516–26. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
