

Endoscopic treatments for Barrett's esophagus: a systematic review of safety and effectiveness compared to esophagectomy
- PMID: 20875123
- PMCID: PMC2955687
- DOI: 10.1186/1471-230X-10-111
Endoscopic treatments for Barrett's esophagus: a systematic review of safety and effectiveness compared to esophagectomy
Abstract
Background: Recently, several new endoscopic treatments have been used to treat patients with Barrett's esophagus with high grade dysplasia. This systematic review aimed to determine the safety and effectiveness of these treatments compared with esophagectomy.
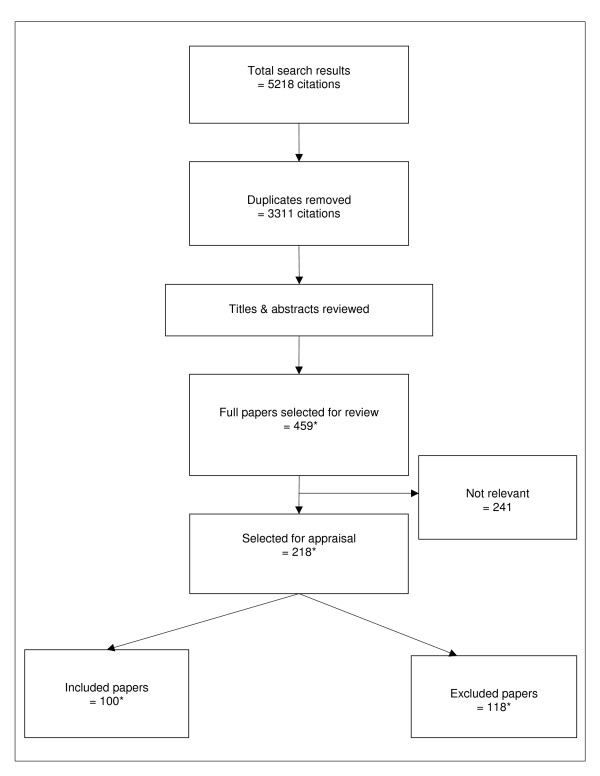
Methods: A comprehensive literature search was undertaken to identify studies of endoscopic treatments for Barrett's esophagus or early stage esophageal cancer. Information from the selected studies was extracted by two independent reviewers. Study quality was assessed and information was tabulated to identify trends or patterns. Results were pooled across studies for each outcome. Safety (occurrence of adverse events) and effectiveness (complete eradication of dysplasia) were compared across different treatments.
Results: The 101 studies that met the selection criteria included 8 endoscopic techniques and esophagectomy; only 12 were comparative studies. The quality of evidence was generally low. Methods and outcomes were inconsistently reported. Protocols, outcomes measured, follow-up times and numbers of treatment sessions varied, making it difficult to calculate pooled estimates.The surgical mortality rate was 1.2%, compared to 0.04% in 2831 patients treated endoscopically (1 death). Adverse events were more severe and frequent with esophagectomy, and included anastomotic leaks (9.4%), wound infections (4.1%) and pulmonary complications (4.1%). Four patients (0.1%) treated endoscopically experienced bleeding requiring transfusions. The stricture rate with esophagectomy (5.3%) was lower than with porfimer sodium photodynamic therapy (18.5%), but higher than aminolevulinic acid (ALA) 60 mg/kg PDT (1.4%). Dysphagia and odynophagia varied in frequency across modalities, with the highest rates reported for multipolar electrocoagulation (MPEC). Photosensitivity, an adverse event that occurs only with photodynamic therapy, was experienced by 26.4% of patients who received porfimer sodium.Some radiofrequency ablation (RFA) or argon plasma coagulation (APC) studies (used in multiple sessions) reported rates of almost 100% for complete eradication of dysplasia. But the study methods and findings were not adequately described. The other studies of endoscopic treatments reported similarly high rates of complete eradication.
Conclusions: Endoscopic treatments offer safe and effective alternatives to esophagectomy for patients with Barrett's esophagus and high grade dysplasia. Unfortunately, shortcomings in the published studies make it impossible to determine the comparative effectiveness of each of the endoscopic treatments.
Figures
Similar articles
-
Treatment for Barrett's oesophagus.Cochrane Database Syst Rev. 2010 Jan 20;2010(1):CD004060. doi: 10.1002/14651858.CD004060.pub2. Cochrane Database Syst Rev. 2010. Retraction in: Cochrane Database Syst Rev. 2021 Mar 4;3:CD004060. doi: 10.1002/14651858.CD004060.pub3. PMID: 20091557 Free PMC article. Retracted.
-
A systematic review of photodynamic therapy in the treatment of pre-cancerous skin conditions, Barrett's oesophagus and cancers of the biliary tract, brain, head and neck, lung, oesophagus and skin.Health Technol Assess. 2010 Jul;14(37):1-288. doi: 10.3310/hta14370. Health Technol Assess. 2010. PMID: 20663420
-
Surveillance of Barrett's oesophagus: exploring the uncertainty through systematic review, expert workshop and economic modelling.Health Technol Assess. 2006 Mar;10(8):1-142, iii-iv. doi: 10.3310/hta10080. Health Technol Assess. 2006. PMID: 16545207
-
Effectiveness, safety, and cost-effectiveness of photodynamic therapy in Barrett's esophagus: a systematic review.Dis Esophagus. 2010 Nov;23(8):633-40. doi: 10.1111/j.1442-2050.2010.01078.x. Dis Esophagus. 2010. PMID: 20545970
-
Endoscopic eradication therapy for mucosal neoplasia in Barrett's esophagus.Curr Opin Gastroenterol. 2013 Jul;29(4):446-53. doi: 10.1097/MOG.0b013e3283622848. Curr Opin Gastroenterol. 2013. PMID: 23703368
Cited by
-
Recent advances in understanding and preventing oesophageal cancer.F1000Res. 2020 Apr 21;9:F1000 Faculty Rev-276. doi: 10.12688/f1000research.21971.1. eCollection 2020. F1000Res. 2020. PMID: 32399195 Free PMC article. Review.
-
Treatment of dysplasia in barrett esophagus.Clin Endosc. 2014 Jan;47(1):55-64. doi: 10.5946/ce.2014.47.1.55. Epub 2014 Jan 24. Clin Endosc. 2014. PMID: 24570884 Free PMC article. Review.
-
Ablative therapy for esophageal dysplasia and early malignancy: focus on RFA.Biomed Res Int. 2014;2014:642063. doi: 10.1155/2014/642063. Epub 2014 Jul 21. Biomed Res Int. 2014. PMID: 25140320 Free PMC article. Review.
-
Photodynamic therapy (PDT) using HPPH for the treatment of precancerous lesions associated with Barrett's esophagus.Lasers Surg Med. 2011 Sep;43(7):705-12. doi: 10.1002/lsm.21112. Lasers Surg Med. 2011. PMID: 22057498 Free PMC article. Clinical Trial.
-
Evolving changes in the management of early oesophageal adenocarcinoma in a tertiary centre.Ir J Med Sci. 2013 Sep;182(3):363-9. doi: 10.1007/s11845-012-0890-x. Epub 2012 Dec 16. Ir J Med Sci. 2013. PMID: 23242575
References
-
- Tougas G, Chen Y, Hwang P, Liu MM, Eggleston A. Prevalence and impact of upper gastrointestinal symptoms in the Canadian population: findings from the DIGEST study. Domestic/International Gastroenterology Surveillance Study. Am J Gastroenterol. 1999;94:2845–2854. doi: 10.1111/j.1572-0241.1999.01427.x. - DOI - PubMed
-
- Esquivel RF, Boolchang V, Kumar N, Camargo L, Kim JL, Fass R, Sampliner RE. The prevalence of Barrett's esophagus in veteran patients with and without GERD symptoms undergoing outpatient colonoscopy [abstract] Gastrointest Endosc. 2008;67:AB172. doi: 10.1016/j.gie.2008.03.402. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
