

Is patent foramen ovale a modifiable risk factor for stroke recurrence?
- PMID: 20876498
- PMCID: PMC2954503
- DOI: 10.1161/STROKEAHA.110.595140
Is patent foramen ovale a modifiable risk factor for stroke recurrence?
Abstract
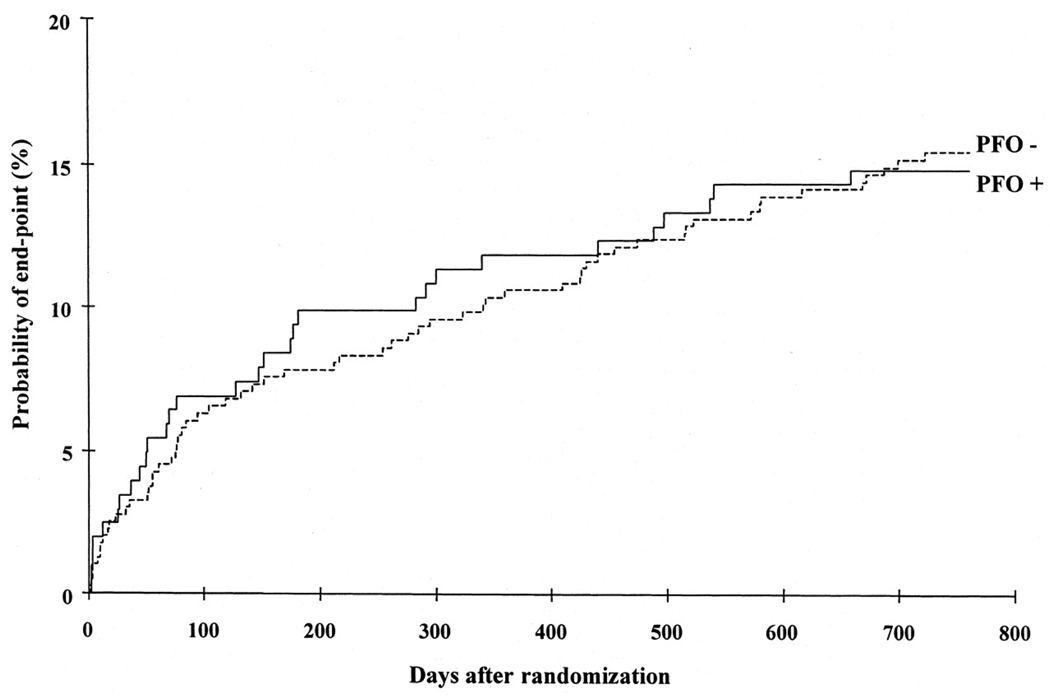
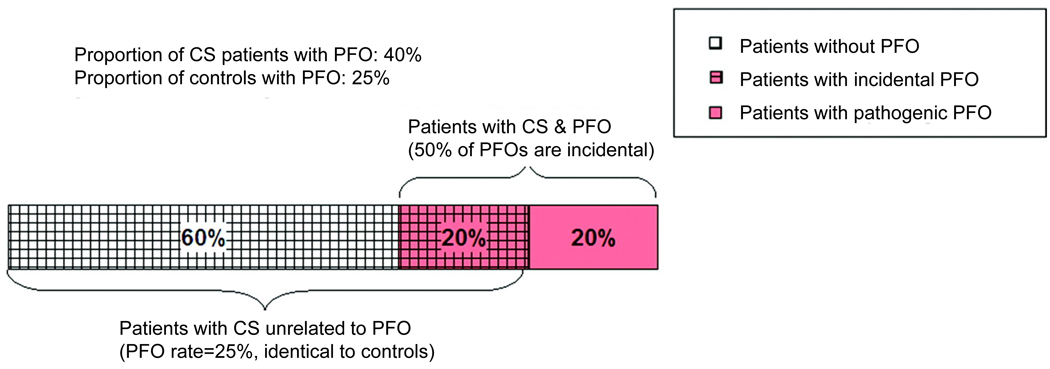
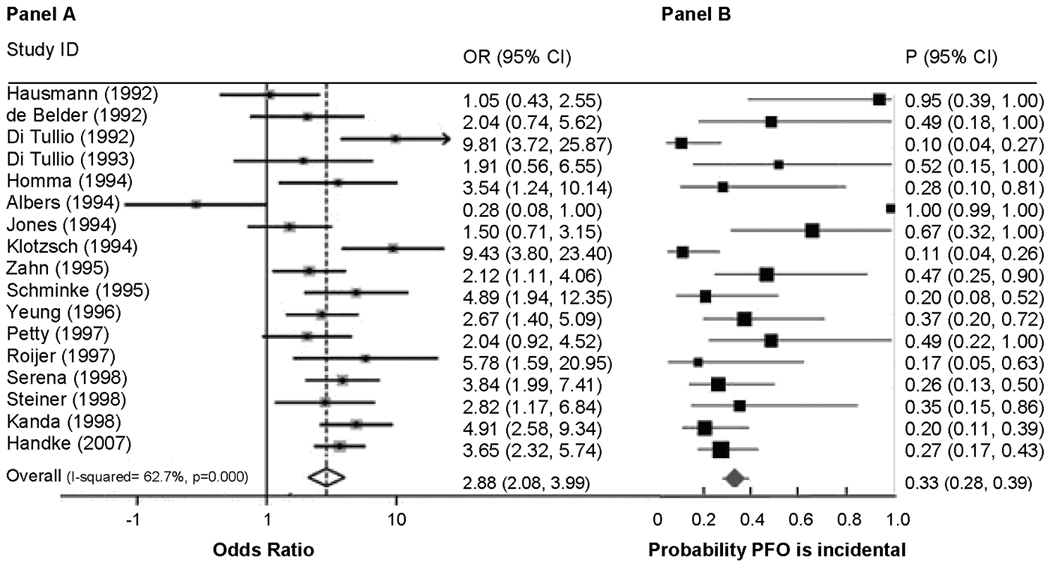
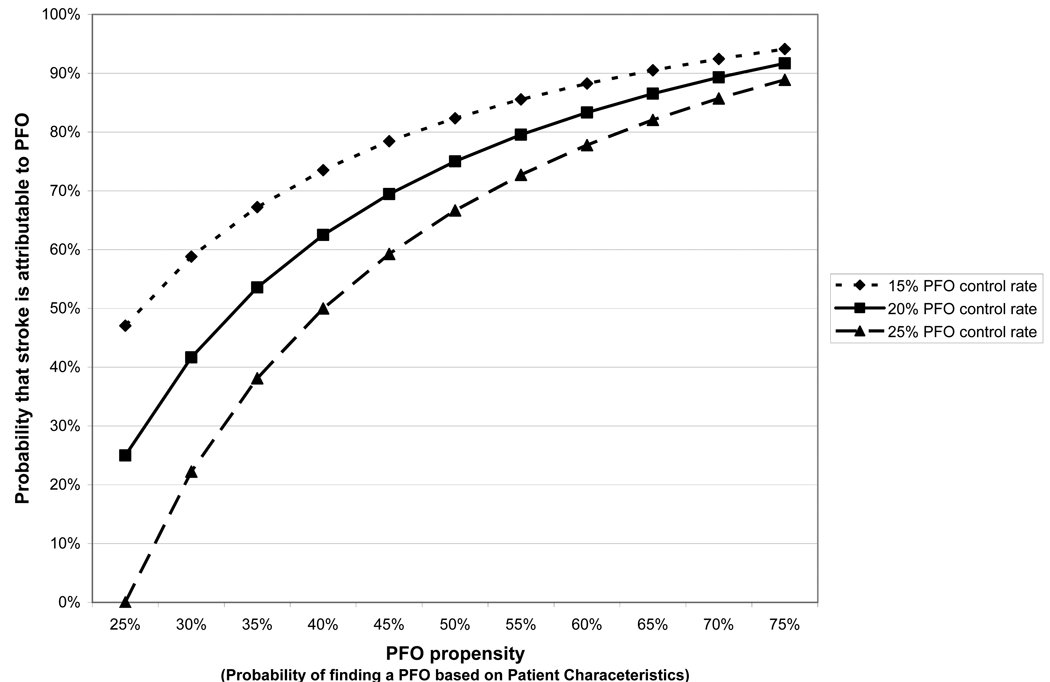
Although the prevalence of a patent foramen ovale (PFO) in the general population is ≈25%, it is approximately doubled among cryptogenic stroke (CS) patients. This has generally been attributed to paradoxical embolism, and many physicians recommend PFO closure to prevent recurrence. However, the benefit of PFO closure in patients with stroke has not been demonstrated. Furthermore, the epidemiology of stroke recurrence in patients with CS with PFO versus without PFO and in those with large right-to-left shunts versus small right-to-left shunts has yielded results that appear difficult to reconcile with the hypothesis that paradoxical embolism is an important cause of stroke recurrence. The purpose of this review is to critically examine the epidemiologic evidence that PFO is a potentially modifiable risk factor for stroke recurrence in patients with CS. The evidence suggests that many patients with CS and PFO have strokes that are PFO attributable, but many have strokes that are unrelated to their PFO. We introduce the concept of "PFO propensity," defined as the patient-specific probability of finding a PFO in a patient with CS on the basis of age and other risk factors. We show that this value is directly related to the probability that CS is PFO attributable. Because there is substantial heterogeneity in both PFO propensity and recurrence risk among patients with PFO and CS, stratification for PFO closure by these joint probabilities will likely prove crucial for appropriate patient selection.
Figures
References
-
- Meissner I, Khandheria BK, Heit JA, Petty GW, Sheps SG, Schwartz GL, Whisnant JP, Wiebers DO, Covalt JL, Petterson TM, Christianson TJ, Agmon Y. Patent foramen ovale: innocent or guilty? Evidence from a prospective population-based study. J Am Coll Cardiol. 2006 January 17;47(2):440–445. - PubMed
-
- Tong DC, Becker KJ. Patent foramen ovale and recurrent stroke: closure is the best option: no. Stroke. 2004 March;35(3):804–805. - PubMed
-
- Homma S, Sacco RL. Patent foramen ovale and stroke. Circulation. 2005 August 16;112(7):1063–1072. - PubMed
-
- Homma S, Sacco RL, Di Tullio MR, Sciacca RR, Mohr JP. Effect of medical treatment in stroke patients with patent foramen ovale: patent foramen ovale in Cryptogenic Stroke Study. Circulation. 2002 June 4;105(22):2625–2631. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
