

Choice of vascular access among incident hemodialysis patients: a decision and cost-utility analysis
- PMID: 20876675
- PMCID: PMC2994091
- DOI: 10.2215/CJN.03210410
Choice of vascular access among incident hemodialysis patients: a decision and cost-utility analysis
Abstract
Background and objectives: Arteriovenous fistulas (AVFs) are widely accepted as the preferred hemodialysis vascular access type. However, supporting data have failed to consider morbidity and mortality incurred during failed creation attempts and may therefore overstate potential advantages. This study compares survival, quality-adjusted survival, and costs among incident hemodialysis patients after attempted placement of AVFs or arteriovenous grafts (AVGs).
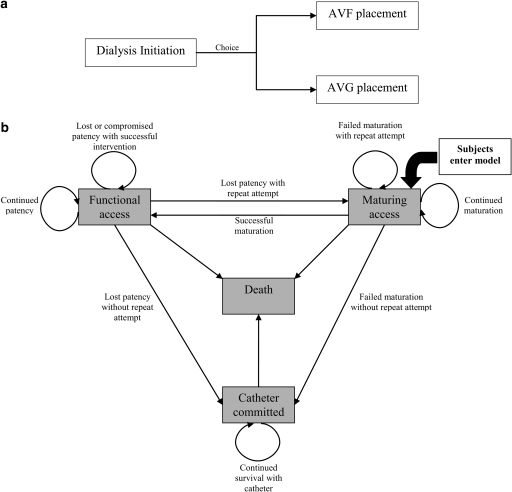
Design, setting, participants, & measurements: Analogous Markov models were created, one each for AVF and AVG. Patients entered consideration at the time of first access creation, contemporaneous with dialysis initiation. Subsequent outcomes were determined probabilistically; transition probabilities, utilities, and costs were gathered from published sources. To ensure comparability between AVFs and AVGs, the timing and likelihood of access maturation were measured in a contemporary cohort of incident hemodialysis patients.
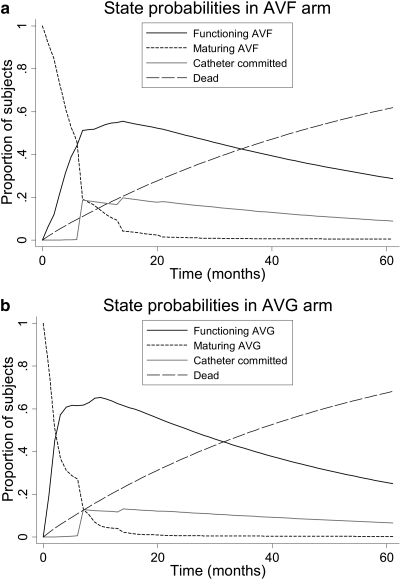
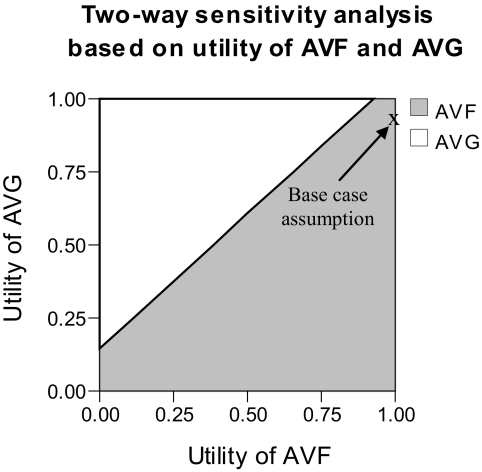
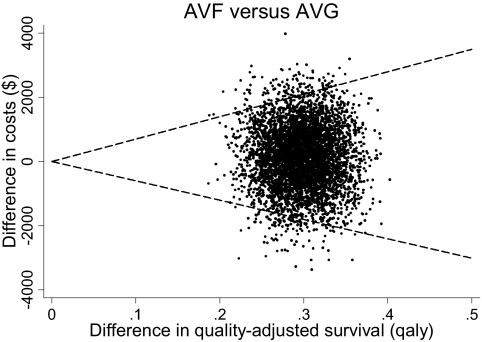
Results: Mean (SD) overall survival was 39.2 (0.8) and 36.7 (1.0) months for AVFs and AVGs, respectively: difference (95% confidence interval [CI]) 2.6 (1.8, 3.3) months. Quality-adjusted survival was 36.1 (0.8) and 32.5 (0.9) quality-adjusted life months (QALMs) for AVFs and AVGs, respectively: difference (95% CI) 3.6 (2.8, 4.3) QALMs. The incremental cost-effectiveness ratio (95% CI) for AVFs relative to AVGs was $446 (-6023, 6994) per quality-adjusted life year saved.
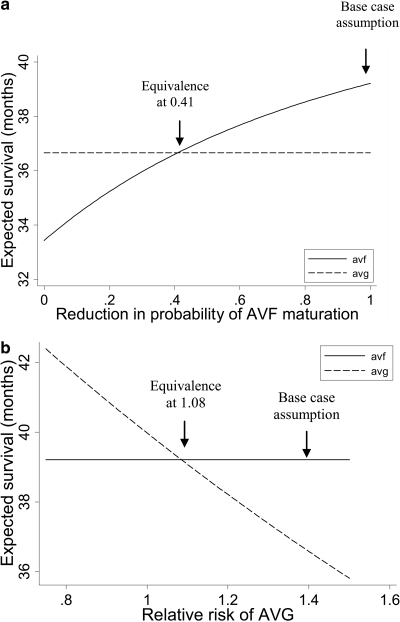
Conclusions: AVFs are associated with greater overall and quality-adjusted survival than AVGs. Observed differences were much less pronounced than might be expected from existing literature, suggesting that prospective identification of patients at high risk for AVF maturational failure might enable improvements in health outcomes via individualization of access planning.
Figures
References
-
- National Kidney Foundation Kidney Disease Outcomes Quality Initiative Guidelines: Clinical Practice Guidelines and Clinical Practice Recommendations: Bethesda, MD, National Kidney Foundation, 2006
-
- Tordoir J, Canaud B, Haage P, Konner K, Basci A, Fouque D, Kooman J, Martin-Malo A, Pedrini L, Pizzarelli F, Tattersall T, Vennegoor M, Wanner C, ter Wee P, Vanholder R: EBPG on vascular access. Nephrol Dial Transplant 22[Suppl 2]: ii88–ii117, 2007 - PubMed
-
- Bradbury BD, Fissell RB, Albert JM, Anthony MS, Critchlow CW, Pisoni RL, Port FK, Gillespie BW: Predictors of early mortality among incident U.S. hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS). Clin J Am Soc Nephrol 2: 89–99, 2007 - PubMed
-
- Ishani A, Collins AJ, Herzog CA, Foley RN: Septicemia, access and cardiovascular disease in dialysis patients: The USRDS Wave 2 study. Kidney Int 68: 311–318, 2005 - PubMed
-
- Astor BC, Eustace JA, Powe NR, Klag MJ, Fink NE, Coresh J: Type of vascular access and survival among incident hemodialysis patients: The Choices for Healthy Outcomes in Caring for ESRD (CHOICE) Study. J Am Soc Nephrol 16: 1449–1455, 2005 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
