

Dialysis practices that distinguish facilities with below- versus above-expected mortality
- PMID: 20876677
- PMCID: PMC3001761
- DOI: 10.2215/CJN.01620210
Dialysis practices that distinguish facilities with below- versus above-expected mortality
Abstract
Background and objectives: Mortality rates vary widely among dialysis facilities even after adjustment with standardized mortality ratios (SMRs). This variation may occur because top-performing facilities use practices not shared by others, because the SMR fails to capture key patient characteristics, or both. Practices were identified that distinguish top- from bottom-performing facilities by SMR.
Design, setting, participants, & measurements: A cross-sectional survey was performed of staff across three organizations. Staff members rated the perceived quality of their units' patient-, provider-, and facility-level practices using a six-point Likert scale. Facilities were divided into those with above- versus below-expected mortality on the basis of SMRs from U.S. Renal Data Service facility reports. Mean Likert scores were computed for each practice using t tests. Practices that were statistically significant (P ≤ 0.05) and achieved at least a medium effect size of ≥0.4 were reported. Significant predictors were entered into a linear regression model.
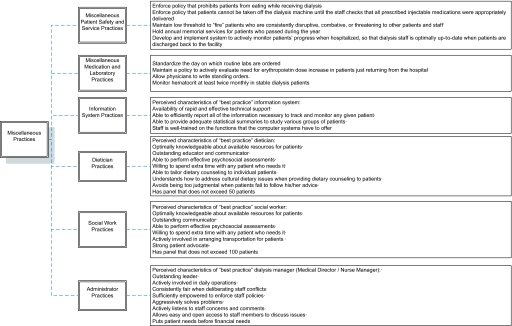
Results: Dialysis facilities with below-expected mortality reported that patients in their unit were more activated and engaged, physician communication and interpersonal relationships were stronger, dieticians were more resourceful and knowledgeable, and overall coordination and staff management were superior versus facilities with above-expected mortality. Staff ratings of these practices explained 31% of the variance in SMRs.
Conclusions: Patient-, provider-, and facility-level practices partly explain SMR variation among facilities. Improving SMRs may require processes that reflect a coordinated, multidisciplinary environment (i.e., no one group, practice, or characteristic will drive facility-level SMRs). Understanding and improving SMRs will require a holistic view of the facility.
Figures



Comment in
-
Processes of care and reduced mortality among hemodialysis patients in the United States.Clin J Am Soc Nephrol. 2010 Nov;5(11):1905-7. doi: 10.2215/CJN.08520910. Epub 2010 Oct 14. Clin J Am Soc Nephrol. 2010. PMID: 20947787 No abstract available.
Similar articles
-
Processes of care and reduced mortality among hemodialysis patients in the United States.Clin J Am Soc Nephrol. 2010 Nov;5(11):1905-7. doi: 10.2215/CJN.08520910. Epub 2010 Oct 14. Clin J Am Soc Nephrol. 2010. PMID: 20947787 No abstract available.
-
Dialysis practices that distinguish top- versus bottom-performing facilities by hemoglobin outcomes.Am J Kidney Dis. 2010 Jul;56(1):86-94. doi: 10.1053/j.ajkd.2010.02.346. Epub 2010 May 20. Am J Kidney Dis. 2010. PMID: 20493604 Clinical Trial.
-
Identifying best practices in dialysis care: results of cognitive interviews and a national survey of dialysis providers.Clin J Am Soc Nephrol. 2008 Jul;3(4):1066-76. doi: 10.2215/CJN.04421007. Epub 2008 Apr 16. Clin J Am Soc Nephrol. 2008. PMID: 18417745 Free PMC article.
-
Patient and facility safety in hemodialysis: opportunities and strategies to develop a culture of safety.Clin J Am Soc Nephrol. 2012 Apr;7(4):680-8. doi: 10.2215/CJN.06530711. Epub 2012 Jan 26. Clin J Am Soc Nephrol. 2012. PMID: 22282480 Free PMC article. Review.
-
The medical director in integrated clinical care models.Clin J Am Soc Nephrol. 2015 Jul 7;10(7):1282-6. doi: 10.2215/CJN.05120514. Epub 2014 Oct 28. Clin J Am Soc Nephrol. 2015. PMID: 25352380 Free PMC article. Review.
Cited by
-
Value-based integrated (renal) care: setting a development agenda for research and implementation strategies.BMC Health Serv Res. 2016 Aug 2;16:330. doi: 10.1186/s12913-016-1586-0. BMC Health Serv Res. 2016. PMID: 27481044 Free PMC article. Review.
-
Risk Adjustment and the Assessment of Disparities in Dialysis Mortality Outcomes.J Am Soc Nephrol. 2015 Nov;26(11):2641-5. doi: 10.1681/ASN.2014050512. Epub 2015 Apr 16. J Am Soc Nephrol. 2015. PMID: 25882829 Free PMC article.
-
Patient Care Technician Staffing and Outcomes Among US Patients Receiving In-Center Hemodialysis.JAMA Netw Open. 2024 Mar 4;7(3):e241722. doi: 10.1001/jamanetworkopen.2024.1722. JAMA Netw Open. 2024. PMID: 38457178 Free PMC article.
-
Health self-assessment by hemodialysis patients in the Brazilian Unified Health System.Rev Saude Publica. 2016;50:10. doi: 10.1590/S1518-8787.2016050005885. Epub 2016 May 3. Rev Saude Publica. 2016. PMID: 27143610 Free PMC article.
-
Predictors of haemoglobin levels and resistance to erythropoiesis-stimulating agents in patients treated with low-flux haemodialysis, haemofiltration and haemodiafiltration: results of a multicentre randomized and controlled trial.Nephrol Dial Transplant. 2012 Sep;27(9):3594-600. doi: 10.1093/ndt/gfs117. Epub 2012 May 23. Nephrol Dial Transplant. 2012. PMID: 22622452 Free PMC article. Clinical Trial.
References
-
- Wolfe RA: The standardized mortality ratio revisited: Improvements, innovations, and limitations. Am J Kidney Dis 24: 290–297, 1994 - PubMed
-
- Wolfe RA, Held PJ, Port FK: Calculation and public use of the unit-specific standardized mortality ratio. Am J Kidney Dis 38: 212–213, 2001 - PubMed
-
- Centers for Medicare and Medicaid Services Dialysis facility compare. Available at: http://www.medicare.gov/Dialysis/Include/DataSection/Questions/SearchCri... Accessed May 1, 2010
-
- McClellan WM, Flanders WD, Gutman RA: Variable mortality rates among dialysis treatment centers. Ann Intern Med 117: 332–336, 1992 - PubMed
-
- Goodkin D: Does case mix explain the differences in dialysis mortality rates around the world? A report from the Dialysis Outcomes and Practice Patterns Study (DOPPS). IKidney—Nephrology Incite. Spring: 2005. (13)
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
