

Mass spectrometry-based proteomic diagnosis of renal immunoglobulin heavy chain amyloidosis
- PMID: 20876678
- PMCID: PMC2994078
- DOI: 10.2215/CJN.02890310
Mass spectrometry-based proteomic diagnosis of renal immunoglobulin heavy chain amyloidosis
Abstract
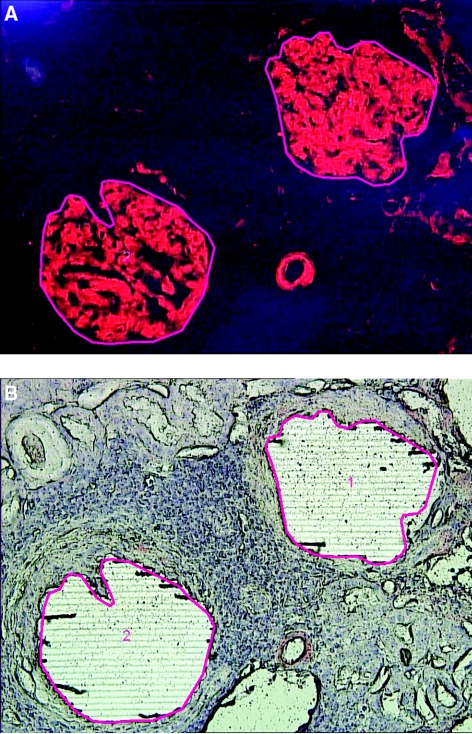
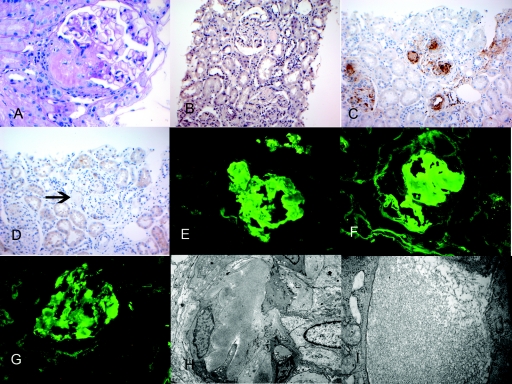
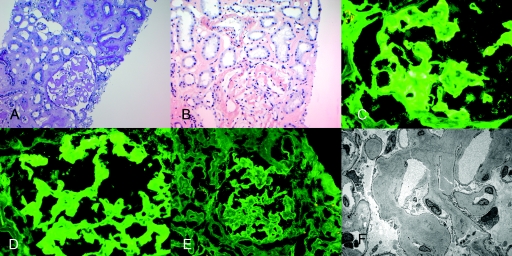
Background and objectives: Amyloidosis is a group of disorders characterized by accumulation of extracellular deposition of proteins as insoluble aggregates. The clinical management of amyloidosis is based on identifying the underlying etiology and accurate typing of the amyloid. Ig heavy chain amyloid involving the kidney is poorly recognized and often poses a diagnostic dilemma. DESIGN, SETTING, PARTICIPANTS, & MEASURES: In this study, we describe the use of laser microdissection (LMD) and mass spectrometry (MS)-based proteomic analysis for the accurate typing of 14 cases of amyloidosis. We also describe the clinicopathologic findings of four problematic cases of renal Ig heavy chain amyloidosis that required LMD/MS proteomic analysis for accurate typing of the amyloid.
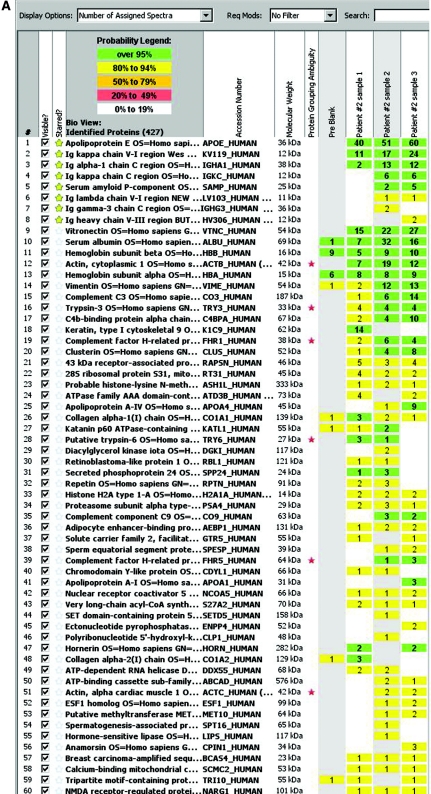
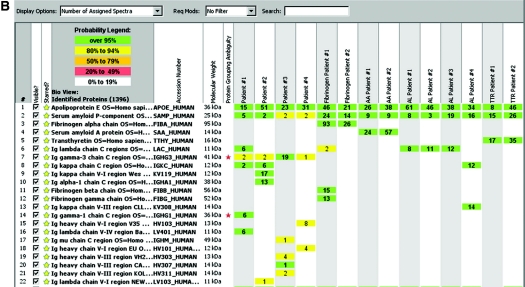
Results: LMD/MS proteomic data of four cases of Ig heavy chain renal amyloidosis showed Ig heavy chains with or without light chains. The break up of the Ig heavy chains was as follows: one case showed Igγ1 chain constant region and λ light chains, one case showed Igα chain constant region and κ light chains variable and constant regions, whereas two cases showed Igγ3 chain constant region and heavy chains variable region I and/or III without light chains. We compare the LMD/MS proteomic data of Ig heavy chain renal amyloid with that of other types of amyloid, including Ig light chains, serum amyloid A, fibrinogen A-α chain renal amyloid, and transthyretin amyloid.
Conclusions: We conclude that LMD/MS is a sensitive and specific tool for diagnosis and accurate typing of renal amyloidosis, including Ig heavy chain amyloid.
Figures
References
-
- Dember LM: Amyloidosis-associated kidney disease. J Am Soc Nephrol 17: 3458–3471, 2006 - PubMed
-
- Merlini G, Bellotti V: Molecular mechanisms of amyloidosis. N Engl J Med 349: 583–596, 2003 - PubMed
-
- Lachmann HJ, Booth DR, Booth SE, Bybee A, Gilbertson JA, Gillmore JD, Pepys MB, Hawkins PN: Misdiagnosis of hereditary amyloidosis as AL (primary) amyloidosis. N Engl J Med 346: 1786–1791, 2002 - PubMed
-
- Miller DV, Dogan A, Sethi S: New-onset proteinuria with massive amorphous glomerular deposits. Am J Kidney Dis 55: 749–754, 2010 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
