

Proliferative glomerulonephritis with monoclonal IgG deposits recurs in the allograft
- PMID: 20876681
- PMCID: PMC3022233
- DOI: 10.2215/CJN.05750710
Proliferative glomerulonephritis with monoclonal IgG deposits recurs in the allograft
Abstract
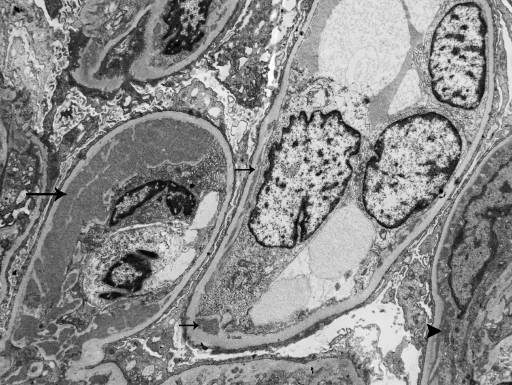
Background and objectives: Proliferative GN with monoclonal IgG deposits (PGNMID) is a newly described entity resembling immune complex GN. Its potential to recur in the allograft is undefined.
Design, setting, participants, & measurements: The first cases of recurrent PGNMID in the allograft are reported.
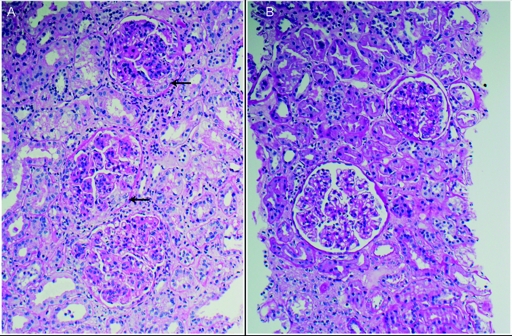
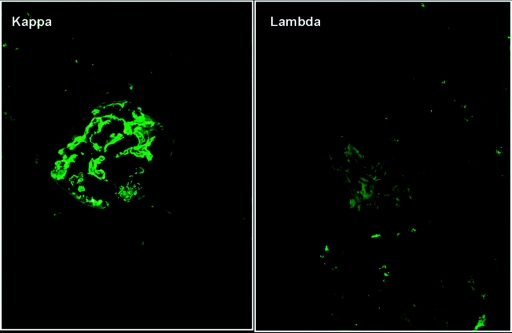
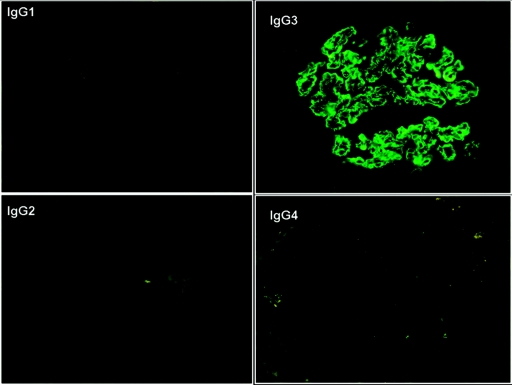
Results: The cohort includes four Caucasians (3 women, 1 man) with a mean age 58.5 years. No patient had M spike or hematologic malignancy. Recurrence was first documented by biopsy at a mean of 3.8 months posttransplant for indications of renal insufficiency in four patients, proteinuria in three patients, and microhematuria in three patients. Monoclonal IgG deposits (3 IgG3κ and 1 IgG3λ) in the transplants had identical heavy- and light-chain isotypes as in the native kidneys. In two patients, a pattern of endocapillary GN was identified in the native and transplant biopsies, whereas two patients with membranoproliferative GN in the native kidney developed endocapillary or mesangial GN in the transplant. Recurrence was treated with combined high-dose prednisone plus rituximab (n = 3) or plus cyclophosphamide (n = 1). After a mean posttransplant follow-up of 43 months, all four patients achieved reduction in proteinuria and three had reduction in creatinine. Repeat biopsies showed reduced histologic activity after treatment.
Conclusions: PGNMID can recur in the transplant despite the absence of a serum M spike. Recurrence is heralded by proteinuria, hematuria, and allograft dysfunction and manifests diverse histologic patterns. Although the pathogenesis remains unknown, early immunosuppressive therapy appears to stabilize the course.
Figures
References
-
- Lin J, Markowitz GS, Valeri AM, Kambham N, Sherman WH, Appel GB, D'Agati VD: Renal monoclonal immunoglobulin deposition disease: The disease spectrum. J Am Soc Nephrol 12: 1482–1492, 2001 - PubMed
-
- Nasr SH, Colvin R, Markowitz GS: IgG1 lambda light and heavy chain renal amyloidosis. Kidney Int 70: 7, 2006 - PubMed
-
- Nasr SH, Markowitz GS, Reddy BS, Maesaka J, Swidler MA, D'Agati VD: Dysproteinemia, proteinuria, and glomerulonephritis. Kidney Int 69: 772–775, 2006 - PubMed
-
- Rosenstock JL, Markowitz GS, Valeri AM, Sacchi G, Appel GB, D'Agati VD: Fibrillary and immunotactoid glomerulonephritis: Distinct entities with different clinical and pathologic features. Kidney Int 63: 1450–1461, 2003 - PubMed
-
- Nasr SH, Markowitz GS, Stokes MB, Seshan SV, Valderrama E, Appel GB, Aucouturier P, D'Agati VD: Proliferative glomerulonephritis with monoclonal IgG deposits: A distinct entity mimicking immune-complex glomerulonephritis. Kidney Int 65: 85–96, 2004 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
