

Abatacept treatment for rheumatoid arthritis
- PMID: 20876701
- PMCID: PMC3042254
- DOI: 10.1093/rheumatology/keq287
Abatacept treatment for rheumatoid arthritis
Abstract
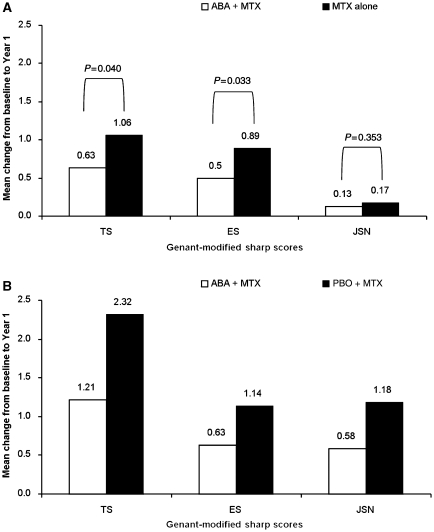
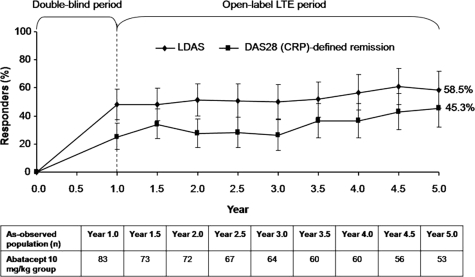
Significant advances in our understanding of RA and its management have been made in the past decade, resulting in earlier intervention with biologic DMARDs, particularly in patients with evidence of aggressive, erosive disease. Here, one such biologic therapy, the T-cell co-stimulation modulator abatacept, is discussed, exploring clinical evidence published to date on its use in patients with very early arthritis/early RA who are MTX naïve, and in patients with established RA and an inadequate response to MTX or TNF antagonists. Data from relevant clinical trials are overviewed, discussing the clinical efficacy of abatacept in early disease, the clinical outcomes over long-term treatment in different patient populations and the effects of abatacept on structural damage. Findings from integrated safety analyses of abatacept clinical trial data, representing 10,366 patient-years of exposure are described, and clinically important safety events, including serious infections, malignancies and autoimmune events, are highlighted. It is concluded that abatacept represents an effective treatment option with an established safety profile across different patient populations, including patients with both early and erosive RA and those with established disease. Furthermore, efficacy data from studies in patients with early disease suggest that the risk-benefit profile of abatacept may be more favourable when introduced earlier in the treatment paradigm.
Figures

References
-
- Landewe RB, Boers M, Verhoeven AC, et al. COBRA combination therapy in patients with early rheumatoid arthritis: long-term structural benefits of a brief intervention. Arthritis Rheum. 2002;46:347–56. - PubMed
-
- O’Dell JR, Leff R, Paulsen G, et al. Treatment of rheumatoid arthritis with methotrexate and hydroxychloroquine, methotrexate and sulfasalazine, or a combination of the three medications: results of a two-year, randomized, double-blind, placebo-controlled trial. Arthritis Rheum. 2002;46:1164–70. - PubMed
-
- Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, et al. Clinical and radiographic outcomes of four different treatment strategies in patients with early rheumatoid arthritis (the BeSt study): a randomized, controlled trial. Arthritis Rheum. 2008;58:S126–35. - PubMed
-
- St Clair EW, van der Heijde DM, Smolen JS, et al. Combination of infliximab and methotrexate therapy for early rheumatoid arthritis: a randomized, controlled trial. Arthritis Rheum. 2004;50:3432–43. - PubMed
-
- Klareskog L, van der Heijde D, de Jager JP, et al. Therapeutic effect of the combination of etanercept and methotrexate compared with each treatment alone in patients with rheumatoid arthritis: double-blind randomised controlled trial. Lancet. 2004;363:675–81. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
