

Three-dimensional susceptibility-weighted imaging and two-dimensional T2*-weighted gradient-echo imaging of intratumoral hemorrhages in pediatric diffuse intrinsic pontine glioma
- PMID: 20878319
- PMCID: PMC3519386
- DOI: 10.1007/s00234-010-0771-9
Three-dimensional susceptibility-weighted imaging and two-dimensional T2*-weighted gradient-echo imaging of intratumoral hemorrhages in pediatric diffuse intrinsic pontine glioma
Abstract
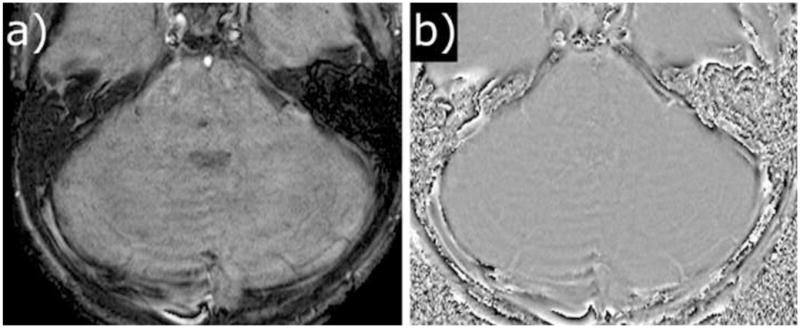
Introduction: We compared the sensitivity and specificity of T2*-weighted gradient-echo imaging (T2*-GRE) and susceptibility-weighted imaging (SWI) in determining prevalence and cumulative incidence of intratumoral hemorrhages in children with diffuse intrinsic pontine glioma (DIPG) undergoing antiangiogenic and radiation therapy.
Methods: Patients were recruited from an institutional review board-approved prospective phase I trial of vandetanib administered in combination with radiation therapy. Patient consent was obtained before enrollment. Consecutive T2*-GRE and SWI exams of 17 patients (F/M: 9/8; age 3-17 years) were evaluated. Two reviewers (R1 and R2) determined the number and size of hemorrhages at baseline and multiple follow-ups (92 scans, mean 5.4/patient). Statistical analyses were performed using descriptive statistics, graphical tools, and mixed-effects Poisson regression models.
Results: Prevalence of hemorrhages at diagnosis was 41% and 47%; the cumulative incidences of hemorrhages at 6 months by T2*-GRE and SWI were 82% and 88%, respectively. Hemorrhages were mostly petechial; 9.7% of lesions on T2*-GRE and 5.2% on SWI were hematomas (>5 mm). SWI identified significantly more hemorrhages than T2*-GRE did. Lesions were missed or misinterpreted in 36/39 (R1/R2) scans by T2*-GRE and 9/3 scans (R1/R2) by SWI. Hemorrhages had no clinically significant neurological correlates in patients.
Conclusions: SWI is more sensitive than T2*-GRE in detecting hemorrhages and differentiating them from calcification, necrosis, and artifacts. Also, petechial hemorrhages are more common in DIPG at diagnosis than previously believed and their number increases during the course of treatment; hematomas are rare.
Conflict of interest statement
Dr. Alberto Broniscer received the study medication from AstraZeneca. All other authors declare that they have no conflict of interest.
Figures






Similar articles
-
Quantitative diffusion-weighted and dynamic susceptibility-weighted contrast-enhanced perfusion MR imaging analysis of T2 hypointense lesion components in pediatric diffuse intrinsic pontine glioma.AJNR Am J Neuroradiol. 2011 Feb;32(2):315-22. doi: 10.3174/ajnr.A2277. Epub 2010 Nov 18. AJNR Am J Neuroradiol. 2011. PMID: 21087935 Free PMC article.
-
Accuracy of SWI sequences compared to T2*-weighted gradient echo sequences in the detection of cerebral cavernous malformations in the familial form.Neuroradiol J. 2016 Oct;29(5):326-35. doi: 10.1177/1971400916665376. Epub 2016 Aug 22. Neuroradiol J. 2016. PMID: 27549150 Free PMC article.
-
Validation of Highly Accelerated Wave-CAIPI SWI Compared with Conventional SWI and T2*-Weighted Gradient Recalled-Echo for Routine Clinical Brain MRI at 3T.AJNR Am J Neuroradiol. 2019 Dec;40(12):2073-2080. doi: 10.3174/ajnr.A6295. Epub 2019 Nov 14. AJNR Am J Neuroradiol. 2019. PMID: 31727749 Free PMC article.
-
Diagnostic performance of T2* gradient echo, susceptibility-weighted imaging, and quantitative susceptibility mapping for patients with multiple system atrophy-parkinsonian type: a systematic review and meta-analysis.Eur Radiol. 2022 Jan;32(1):308-318. doi: 10.1007/s00330-021-08174-4. Epub 2021 Jul 16. Eur Radiol. 2022. PMID: 34272590
-
[Diagnostic imaging of hemangiomas in the brain].Brain Nerve. 2011 Jan;63(1):5-15. Brain Nerve. 2011. PMID: 21228443 Review. Japanese.
Cited by
-
Computational Fractal-Based Analysis of MR Susceptibility-Weighted Imaging (SWI) in Neuro-Oncology and Neurotraumatology.Adv Neurobiol. 2024;36:445-468. doi: 10.1007/978-3-031-47606-8_23. Adv Neurobiol. 2024. PMID: 38468047
-
MRI-based radiomics for prognosis of pediatric diffuse intrinsic pontine glioma: an international study.Neurooncol Adv. 2021 Mar 5;3(1):vdab042. doi: 10.1093/noajnl/vdab042. eCollection 2021 Jan-Dec. Neurooncol Adv. 2021. PMID: 33977272 Free PMC article.
-
MRI Evaluation of Non-Necrotic T2-Hyperintense Foci in Pediatric Diffuse Intrinsic Pontine Glioma.AJNR Am J Neuroradiol. 2016 Oct;37(10):1930-1937. doi: 10.3174/ajnr.A4814. Epub 2016 May 19. AJNR Am J Neuroradiol. 2016. PMID: 27197987 Free PMC article.
-
Advanced Imaging Techniques for Newly Diagnosed and Recurrent Gliomas.Front Neurosci. 2022 Feb 23;16:787755. doi: 10.3389/fnins.2022.787755. eCollection 2022. Front Neurosci. 2022. PMID: 35281485 Free PMC article. Review.
-
Posterior fossa tumors in children: developmental anatomy and diagnostic imaging.Childs Nerv Syst. 2015 Oct;31(10):1661-76. doi: 10.1007/s00381-015-2834-z. Epub 2015 Sep 9. Childs Nerv Syst. 2015. PMID: 26351220 Review.
References
-
- CBTRUS. Published by the Central Brain Tumor Registry of the United States. 2005. Statistical Report: Primary Brain Tumors in the United States, 1998–2002.
-
- Kaatsch P, Rickert CH, Kuhl L, Schuz J, Michaelis J. Population-based epidemiologic data on brain tumors in German children. Cancer. 2001;92:3155–3164. - PubMed
-
- Fischbein NJ, Prados MD, Wara W, Russo C, Edwards MSB, Barkovich AJ. Radiologic classification of brain stem tumors: Correlation of magnetic resonance imaging appearance with clinical outcome. Pediatr Neurosurg. 1996;24:9–23. - PubMed
-
- Hargrave D, Bartels U, Bouffet E. Diffuse brainstem glioma in children: critical review of clinical trials. Lancet Oncol. 2006;7:241–248. - PubMed
-
- Folkman J, Bach M, Rowe JW, Davidoff F, Lambert P, Hirsch C, Goldberg A, Hiatt HH, Glass J, Henshaw E. Tumor Angiogenesis - Therapeutic Implications. N Engl J Med. 1971;285:1182–1186. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
