

Preoperative concurrent paclitaxel-radiation in locally advanced breast cancer: pathologic response correlates with five-year overall survival
- PMID: 20878462
- PMCID: PMC3655407
- DOI: 10.1007/s10549-010-1181-8
Preoperative concurrent paclitaxel-radiation in locally advanced breast cancer: pathologic response correlates with five-year overall survival
Abstract
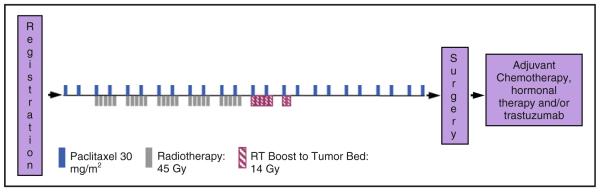
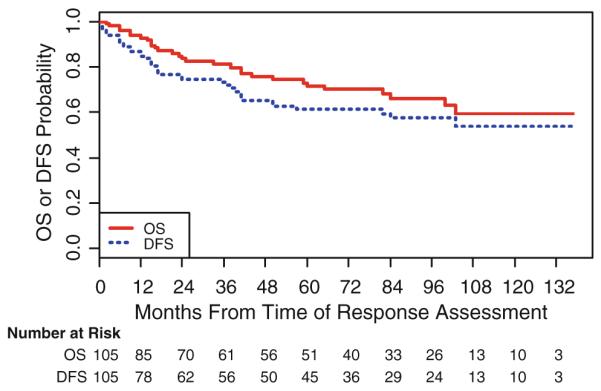
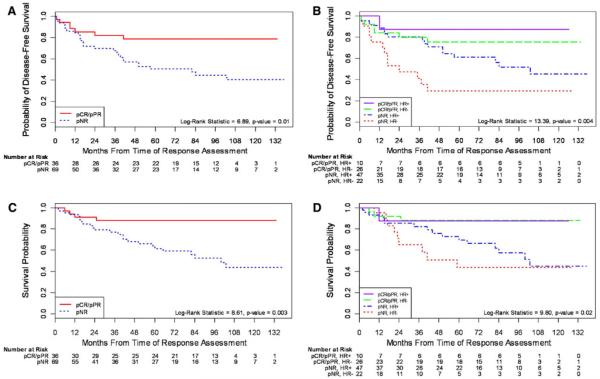
We have previously demonstrated high pathologic response rates after neoadjuvant concurrent chemoradiation in patients with locally advanced breast cancer (LABC). We now report disease-free survival (DFS) and overall survival (OS) in the context of pathologic response. 105 LABC patients (White 46%, Non-White 54%) were treated with paclitaxel (30 mg/m² intravenously twice a week) for 10-12 weeks. Daily radiotherapy was delivered to breast, axillary, and supraclavicular lymph nodes during weeks 2-7 of paclitaxel treatment, at 1.8 Gy per fraction to a total dose of 45 Gy with a tumor boost of 14 Gy at 2 Gy/fraction. Pathological complete response (pCR) was defined as the absence of invasive cancer in breast and lymph nodes and pathological partial response (pPR) as the persistence of <10 microscopic foci of invasive carcinoma in breast or lymph nodes. Pathologic response (pCR and pPR) after neoadjuvant chemoradiation was achieved in 36/105 patients (34%) and was associated with significantly better DFS and OS. Pathological responders had a lower risk of recurrence or death (HR = 0.35, P = 0.01) and a longer OS (HR = 4.27, P = 0.01) compared with non-responders. Median DFS and OS were 57 and 84 months for non-responders, respectively, and have not yet been reached for responders. Importantly, pathologic response was achieved in 54% of patients with HR negative tumors (26/48). In conclusion, pathologic response to concurrent paclitaxel-radiation translated into superior DFS and OS. Half of the patients with HR negative tumors achieved a pathologic response.
Figures
References
-
- Feldman LD, Hortobagyi GN, Buzdar AU, Ames FC, Blumenschein GR. Pathological assessment of response to induction chemotherapy in breast cancer. Cancer Res. 1986;46(5):2578–2581. - PubMed
-
- Rastogi P, Anderson SJ, Bear HD, Geyer CE, Kahlenberg MS, Robidoux A, Margolese RG, Hoehn JL, Vogel VG, Dakhil SR, Tamkus D, King KM, Pajon ER, Wright MJ, Robert J, Paik S, Mamounas EP, Wolmark N. Preoperative chemotherapy: updates of national surgical adjuvant breast and bowel project protocols -18 and b-27. J Clin Oncol. 2008;26(5):778–785. doi:10.1200/JCO.2007.15.0235. - PubMed
-
- Buzdar AU, Ibrahim NK, Francis D, Booser DJ, Thomas ES, Theriault RL, Pusztai L, Green MC, Arun BK, Giordano SH, Cristofanilli M, Frye DK, Smith TL, Hunt KK, Singletary SE, Sahin AA, Ewer MS, Buchholz TA, Berry D, Hortobagyi GN. Significantly higher pathologic complete remission rate after neoadjuvant therapy with trastuzumab, paclitaxel, and epirubicin chemotherapy: results of a randomized trial in human epidermal growth factor receptor 2-positive operable breast cancer. J Clin Oncol. 2005;23(16):3676–3685. doi:10.1200/JCO.2005.07.032. - PubMed
-
- Buzdar AU, Valero V, Ibrahim NK, Francis D, Broglio KR, Theriault RL, Pusztai L, Green MC, Singletary SE, Hunt KK, Sahin AA, Esteva F, Symmans WF, Ewer MS, Buchholz TA, Hortobagyi GN. Neoadjuvant therapy with paclitaxel followed by 5-fluorouracil, epirubicin, and cyclophosphamide chemotherapy and concurrent trastuzumab in human epidermal growth factor receptor 2-positive operable breast cancer: an update of the initial randomized study population and data of additional patients treated with the same regimen. Clin Cancer Res. 2007;13(1):228–233. doi:10.1158/1078-0432.CCR-06-1345. - PubMed
-
- Sikov WM, Dizon DS, Strenger R, Legare RD, Theall KP, Graves TA, Gass JS, Kennedy TA, Fenton MA. Frequent pathologic complete responses in aggressive stages ii to iii breast cancers with every-4-week carboplatin and weekly paclitaxel with or without trastuzumab: a brown university oncology group study. J Clin Oncol. 2009;27(28):4693–4700. doi:10.1200/JCO.2008.21.4163. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- M01 RR000096/RR/NCRR NIH HHS/United States
- T32 CA009385/CA/NCI NIH HHS/United States
- CA138106/CA/NCI NIH HHS/United States
- R01 CA105436/CA/NCI NIH HHS/United States
- CA070856/CA/NCI NIH HHS/United States
- 5P30 CA016037-30/CA/NCI NIH HHS/United States
- R01 CA070856/CA/NCI NIH HHS/United States
- CA009385/CA/NCI NIH HHS/United States
- P30 CA068485/CA/NCI NIH HHS/United States
- CA68485/CA/NCI NIH HHS/United States
- ES00267/ES/NIEHS NIH HHS/United States
- P30 ES000267/ES/NIEHS NIH HHS/United States
- CA105436/CA/NCI NIH HHS/United States
- P30 CA016087/CA/NCI NIH HHS/United States
- F32 CA138106/CA/NCI NIH HHS/United States
- K23CA125205P50/CA/NCI NIH HHS/United States
- K23 CA125205/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
