

Predictive modeling of lung motion over the entire respiratory cycle using measured pressure-volume data, 4DCT images, and finite-element analysis
- PMID: 20879598
- PMCID: PMC2927691
- DOI: 10.1118/1.3455276
Predictive modeling of lung motion over the entire respiratory cycle using measured pressure-volume data, 4DCT images, and finite-element analysis
Abstract
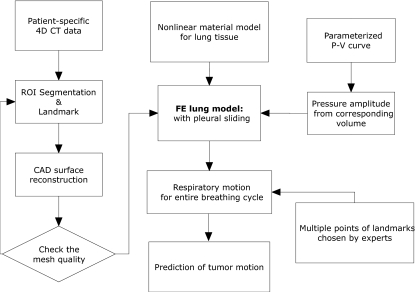
Purpose: Predicting complex patterns of respiration can benefit the management of the respiratory motion for radiation therapy of lung cancer. The purpose of the present work was to develop a patient-specific, physiologically relevant respiratory motion model which is capable of predicting lung tumor motion over a complete normal breathing cycle.
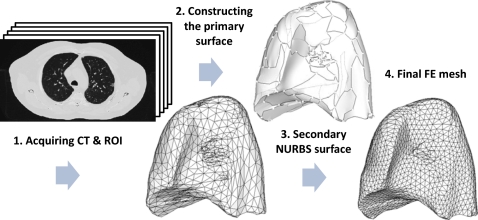
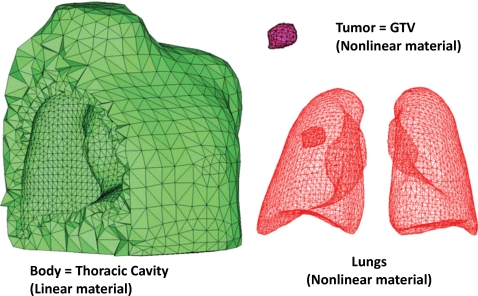
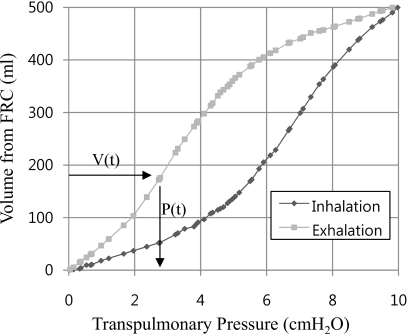
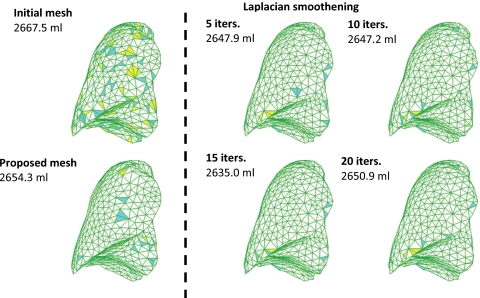
Methods: Currently employed techniques for generating the lung geometry from four-dimensional computed tomography data tend to lose details of mesh topology due to excessive surface smoothening. Some of the existing models apply displacement boundary conditions instead of the intrapleural pressure as the actual motive force for respiration, while others ignore the nonlinearity of lung tissues or the mechanics of pleural sliding. An intermediate nonuniform rational basis spline surface representation is used to avoid multiple geometric smoothing procedures used in the computational mesh preparation. Measured chest pressure-volume relationships are used to simulate pressure loading on the surface of the model for a given lung volume, as in actual breathing. A hyperelastic model, developed from experimental observations, has been used to model the lung tissue material. Pleural sliding on the inside of the ribcage has also been considered.
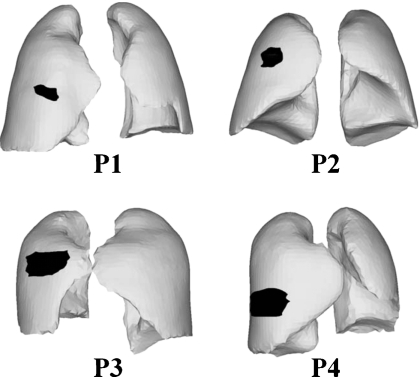
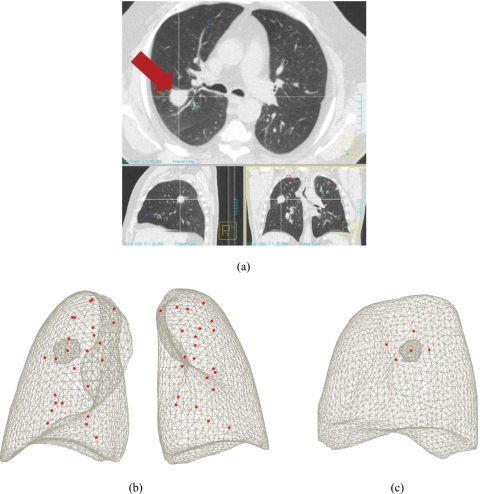
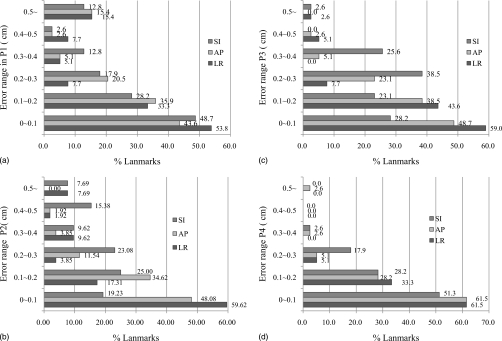
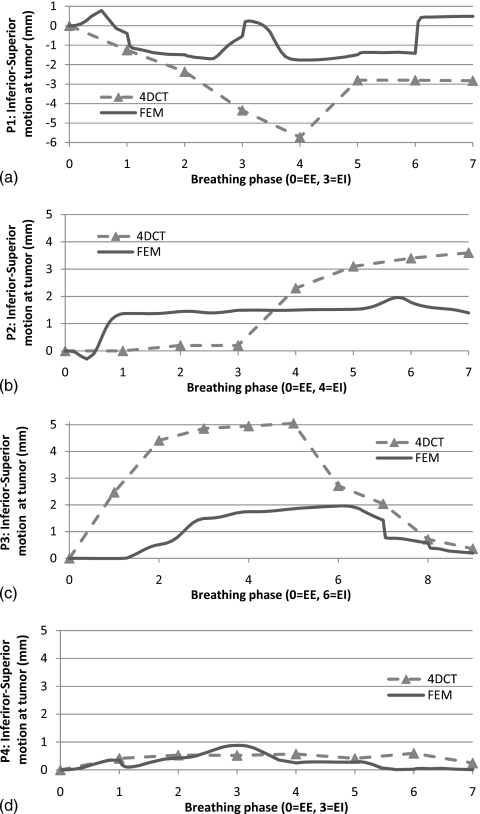
Results: The finite-element model has been validated using landmarks from four patient CT data sets over 34 breathing phases. The average differences of end-inspiration in position between the landmarks and those predicted by the model are observed to be 0.450 +/- 0.330 cm for Patient P1, 0.387 +/- 0.169 cm for Patient P2, 0.319 +/- 0.186 cm for Patient P3, and 0.204 +/- 0.102 cm for Patient P4 in the magnitude of error vector, respectively. The average errors of prediction at landmarks over multiple breathing phases in superior-inferior direction are less than 3 mm.
Conclusions: The prediction capability of pressure-volume curve driven nonlinear finite-element model is consistent over the entire breathing cycle. The biomechanical parameters in the model are physiologically measurable, so that the results can be extended to other patients and additional neighboring organs affected by respiratory motion.
Figures
Similar articles
-
Modeling respiratory motion for cancer radiation therapy based on patient-specific 4DCT data.Med Image Comput Comput Assist Interv. 2009;12(Pt 2):348-55. doi: 10.1007/978-3-642-04271-3_43. Med Image Comput Comput Assist Interv. 2009. PMID: 20426131
-
Patient-specific finite element modeling of respiratory lung motion using 4D CT image data.Med Phys. 2009 May;36(5):1500-11. doi: 10.1118/1.3101820. Med Phys. 2009. PMID: 19544766
-
Tracking lung tissue motion and expansion/compression with inverse consistent image registration and spirometry.Med Phys. 2007 Jun;34(6):2155-63. doi: 10.1118/1.2731029. Med Phys. 2007. PMID: 17654918
-
Developing a Lung Model in the Age of COVID-19: A Digital Image Correlation and Inverse Finite Element Analysis Framework.Front Bioeng Biotechnol. 2021 Oct 26;9:684778. doi: 10.3389/fbioe.2021.684778. eCollection 2021. Front Bioeng Biotechnol. 2021. PMID: 34765590 Free PMC article. Review.
-
Image-based modeling of lung structure and function.J Magn Reson Imaging. 2010 Dec;32(6):1421-31. doi: 10.1002/jmri.22382. J Magn Reson Imaging. 2010. PMID: 21105146 Free PMC article. Review.
Cited by
-
4D Cone-beam CT reconstruction using a motion model based on principal component analysis.Med Phys. 2011 Dec;38(12):6697-709. doi: 10.1118/1.3662895. Med Phys. 2011. PMID: 22149852 Free PMC article.
-
Four-dimensional radiotherapeutic dose calculation using biomechanical respiratory motion description.Int J Comput Assist Radiol Surg. 2014 May;9(3):449-57. doi: 10.1007/s11548-013-0935-2. Epub 2013 Sep 1. Int J Comput Assist Radiol Surg. 2014. PMID: 23996090
-
Evaluation of Malignant Lung Tumor Motion Comparing to Fix Point during Different Respiratory Phases on Four-Dimensional Computed Tomography.Maedica (Bucur). 2024 Sep;19(3):461-469. doi: 10.26574/maedica.2024.19.3.461. Maedica (Bucur). 2024. PMID: 39553348 Free PMC article.
-
Advances in Computational Human Phantoms and Their Applications in Biomedical Engineering - A Topical Review.IEEE Trans Radiat Plasma Med Sci. 2019 Jan;3(1):1-23. doi: 10.1109/TRPMS.2018.2883437. IEEE Trans Radiat Plasma Med Sci. 2019. PMID: 30740582 Free PMC article.
-
The physical basis and future of radiation therapy.Br J Radiol. 2011 Jun;84(1002):485-98. doi: 10.1259/bjr/86221320. Br J Radiol. 2011. PMID: 21606068 Free PMC article. Review.
References
-
- ICRU, “Prescribing, recording and reporting photon beam therapy (supplement to ICRU Report 50),” ICRU Report No. 62 (International Commission on Radiation Units and Measurements, Bethesda, MD, 1999).
-
- Li G., Citrin D., Camphausen K., Mueller B., Burman C., Mychalczak B., Miller R., and Song Y., “Advances in 4D medical imaging and 4D radiation therapy,” Technol. Cancer Res. Treat. TCRTBS 7, 67–81 (2008). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
