

Bilirubin protects grafts against nonspecific inflammation-induced injury in syngeneic intraportal islet transplantation
- PMID: 20881452
- PMCID: PMC2992853
- DOI: 10.3858/emm.2010.42.11.075
Bilirubin protects grafts against nonspecific inflammation-induced injury in syngeneic intraportal islet transplantation
Abstract
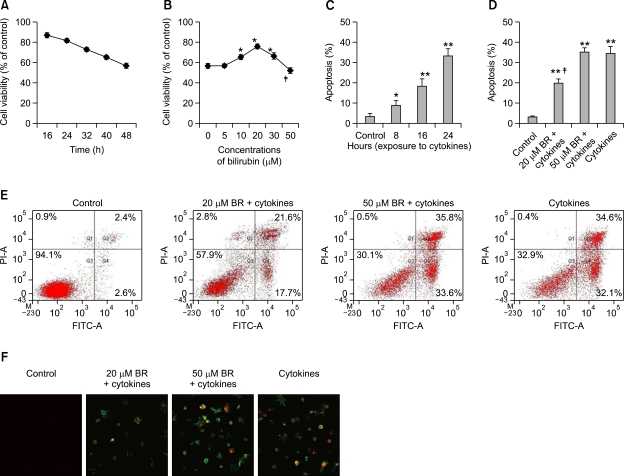
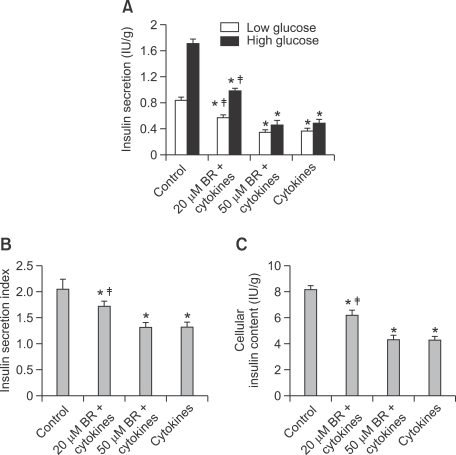
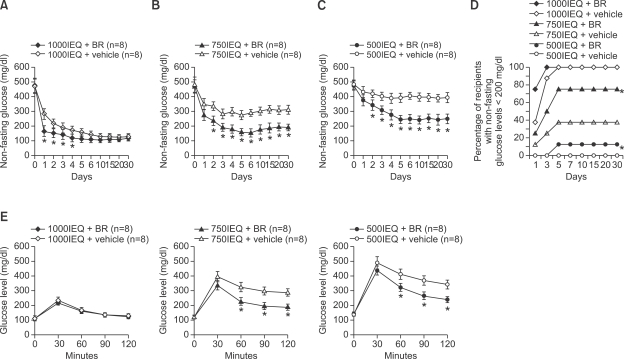
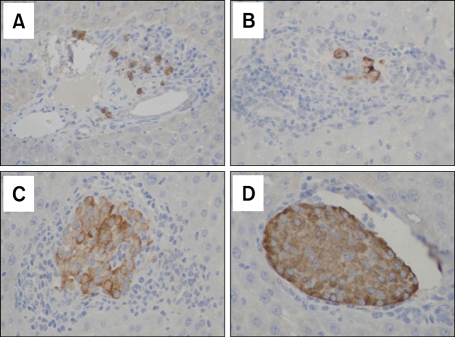
Nonspecific inflammatory response is the major cause for failure of islet grafts at the early phase of intraportal islet transplantation (IPIT). Bilirubin, a natural product of heme catabolism, has displayed anti-oxidative and anti-inflammatory activities. The present study has demonstrated that bilirubin protected islet grafts by inhibiting nonspecific inflammatory response in a syngeneic rat model of IPIT. The inflammation-induced cell injury was mimicked by exposing cultured rat insulinoma INS-1 cells to cytokines (IL-1β, TNF-α and IFN-γ) in in vitro assays. At appropriate lower concentrations, bilirubin significantly attenuated the reduced cell viability and enhanced cell apoptosis induced by cytokines, and protected the insulin secretory function of INS-1 cells. Diabetic inbred male Lewis rats induced by streptozotocin underwent IPIT at different islet equivalents (IEQs) (optimal dose of 1000, and suboptimal doses of 750 or 500), and bilirubin was administered to the recipients every 12 h, starting from one day before transplantation until 5 days after transplantation. Administration of bilirubin improved glucose control and enhanced glucose tolerance in diabetic recipients, and reduced the serum levels of inflammatory mediators including IL-1β, TNF-α, soluble intercellular adhesion molecule 1, monocyte chemoattractant protein-1 and NO, and inhibited the infiltration of Kupffer cells into the islet grafts, and restored insulin-producing ability of transplanted islets.
Figures
Similar articles
-
Interleukin-1beta and inducible form of nitric oxide synthase expression in early syngeneic islet transplantation.J Endocrinol. 2007 Jan;192(1):169-77. doi: 10.1677/joe.1.06968. J Endocrinol. 2007. PMID: 17210754
-
Role of blood glucose in cytokine gene expression in early syngeneic islet transplantation.Cell Transplant. 2007;16(5):517-25. doi: 10.3727/000000007783464920. Cell Transplant. 2007. PMID: 17708341
-
Brain death significantly reduces isolated pancreatic islet yields and functionality in vitro and in vivo after transplantation in rats.Diabetes. 2003 Dec;52(12):2935-42. doi: 10.2337/diabetes.52.12.2935. Diabetes. 2003. PMID: 14633854
-
A Nonhematopoietic Erythropoietin Analogue, ARA 290, Inhibits Macrophage Activation and Prevents Damage to Transplanted Islets.Transplantation. 2016 Mar;100(3):554-62. doi: 10.1097/TP.0000000000001026. Transplantation. 2016. PMID: 26683514
-
Liver ischemia contributes to early islet failure following intraportal transplantation: benefits of liver ischemic-preconditioning.Am J Transplant. 2006 Jan;6(1):60-8. doi: 10.1111/j.1600-6143.2005.01157.x. Am J Transplant. 2006. PMID: 16433757
Cited by
-
Nano-Encapsulation of Bilirubin in Pluronic F127-Chitosan Improves Uptake in β Cells and Increases Islet Viability and Function after Hypoxic Stress.Cell Transplant. 2017 Oct;26(10):1703-1715. doi: 10.1177/0963689717735112. Cell Transplant. 2017. PMID: 29251115 Free PMC article.
-
Pharmaceutical strategies for preventing toxicity and promoting antioxidant and anti-inflammatory actions of bilirubin.J Enzyme Inhib Med Chem. 2022 Dec;37(1):487-501. doi: 10.1080/14756366.2021.2020773. J Enzyme Inhib Med Chem. 2022. PMID: 34986721 Free PMC article. Review.
-
Serum Bilirubin Levels in Overweight and Obese Individuals: The Importance of Anti-Inflammatory and Antioxidant Responses.Antioxidants (Basel). 2021 Aug 26;10(9):1352. doi: 10.3390/antiox10091352. Antioxidants (Basel). 2021. PMID: 34572984 Free PMC article. Review.
-
Prognostic Value of Total Bilirubin in Patients With ST-Segment Elevation Acute Myocardial Infarction Undergoing Primary Coronary Intervention.Front Cardiovasc Med. 2020 Dec 17;7:615254. doi: 10.3389/fcvm.2020.615254. eCollection 2020. Front Cardiovasc Med. 2020. PMID: 33392275 Free PMC article.
-
Bile pigments in pulmonary and vascular disease.Front Pharmacol. 2012 Mar 8;3:39. doi: 10.3389/fphar.2012.00039. eCollection 2012. Front Pharmacol. 2012. PMID: 22408625 Free PMC article.
References
-
- Amoli MM, Larijani B. Would blockage of cytokines improve the outcome of pancreatic islet transplantation? Med Hypotheses. 2006;66:816–819. - PubMed
-
- Arita S, Une S, Ohtsuka S, Atiya A, Kasraie A, Shevlin L, Mullen Y. Prevention of primary islet isograft nonfunction in mice with pravastatin. Transplantation. 1998;65:1429–1433. - PubMed
-
- Biarnés M, Montolio M, Nacher V, Raurell M, Soler J, Montanya E. Beta-cell death and mass in syngeneically transplanted islets exposed to short- and long-term hyperglycemia. Diabetes. 2002;51:66–72. - PubMed
-
- Bottino R, Fernandez LA, Ricordi C, Lehmann R, Tsan MF, Oliver R, Inverardi L. Transplantation of allogeneic islets of Langerhans in the rat liver: effects of macrophage depletion on graft survival and microenvironment activation. Diabetes. 1998;47:316–323. - PubMed
-
- Cantaluppi V, Biancone L, Romanazzi GM, Figliolini F, Beltramo S, Ninniri MS, Galimi F, Romagnoli R, Franchello A, Salizzoni M, Perin PC, Ricordi C, Segoloni GP, Camussi G. Antiangiogenic and immunomodulatory effects of rapamycin on islet endothelium: relevance for islet transplantation. Am J Transplant. 2006;6:2601–2611. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials