

Normothermia to prevent surgical site infections after gastrointestinal surgery: holy grail or false idol?
- PMID: 20881777
- PMCID: PMC3398839
- DOI: 10.1097/SLA.0b013e3181f6c2a9
Normothermia to prevent surgical site infections after gastrointestinal surgery: holy grail or false idol?
Abstract
Objective: To analyze the association between perioperative normothermia (temperature ≥36°C) and surgical site infections (SSIs) after gastrointestinal (GI) surgery.
Summary of background data: Although active warming during colorectal surgery reduces SSIs, there is limited evidence that perioperative normothermia is associated with lower rates of SSI. Nonetheless, hospitals participating in the Surgical Care Improvement Project must report normothermia rates during major surgery.
Methods: We conducted a nested, matched, case-control study; cases consisted of GI surgery patients enrolled in our National Surgical Quality Improvement Program database between March 2006 and March 2009 who developed SSIs. Patient/surgery risk factors for SSI were obtained from the National Surgical Quality Improvement Program database. Perioperative temperature/antibiotic/glucose data were obtained from medical records. Cases/controls were compared using univariate/random effects/logistic regression models. Independent risk factors for SSIs were identified using multivariate/random effects/logistic regression models.
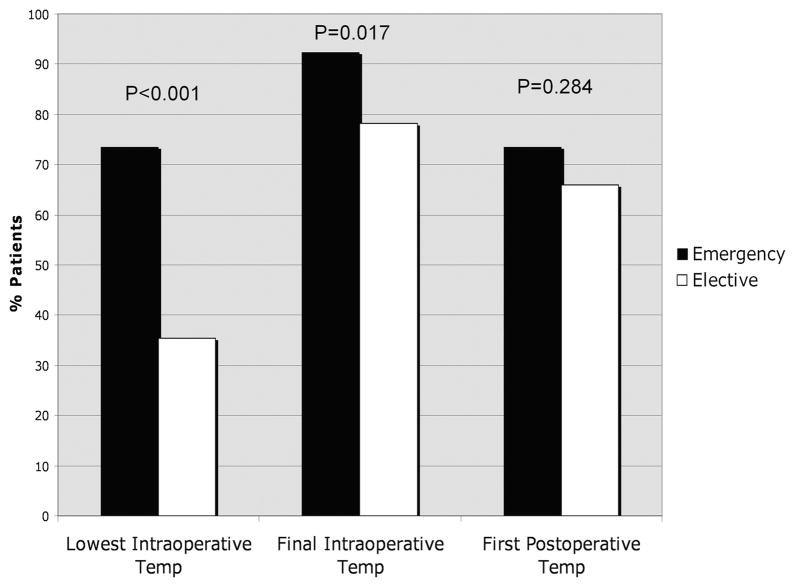
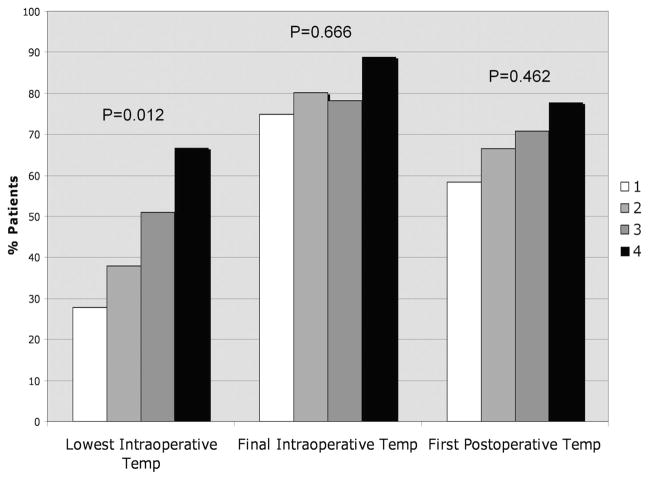
Results: A total of 146 cases and 323 matched controls were identified; 82% of patients underwent noncolorectal surgery. Cases were more likely to have final intraoperative normothermia compared with controls (87.6% vs. 77.8%, P = 0.015); rates of immediate postoperative normothermia were similar (70.6% vs. 65.3%, respectively, P = 0.19). Emergent surgery/higher wound class were associated with higher rates of intraoperative normothermia. Independent risk factors for SSI were diabetes, surgical complexity, small bowel surgery, and nonlaparoscopic surgery. There was no independent association between perioperative normothermia and SSI (adjusted odds ratio, 1.05; 95% confidence interval, 0.48-2.33; P = 0.90).
Conclusions: Pay-for-reporting measures focusing on perioperative normothermia may be of limited value in preventing SSI after GI surgery. Studies to define the benefit of active warming after noncolorectal GI surgery are warranted.
Figures

Comment in
-
Holy grail or false idol-and how to tell the difference.Ann Surg. 2011 Oct;254(4):673-4; author reply 674-5. doi: 10.1097/SLA.0b013e3182306a11. Ann Surg. 2011. PMID: 21892070 No abstract available.
Similar articles
-
Inadvertent perioperative hypothermia and surgical site infections after liver resection.Hepatobiliary Pancreat Dis Int. 2024 Dec;23(6):579-585. doi: 10.1016/j.hbpd.2023.12.006. Epub 2023 Dec 30. Hepatobiliary Pancreat Dis Int. 2024. PMID: 38185585
-
Continuous intraoperative temperature measurement and surgical site infection risk: analysis of anesthesia information system data in 1008 colorectal procedures.Ann Surg. 2013 Oct;258(4):606-12; discussion 612-3. doi: 10.1097/SLA.0b013e3182a4ec0f. Ann Surg. 2013. PMID: 23989047
-
Association Between Normothermia at the End of Surgery and Postoperative Complications Following Orthopedic Surgery.Clin Infect Dis. 2020 Jan 16;70(3):474-482. doi: 10.1093/cid/ciz213. Clin Infect Dis. 2020. PMID: 30863863
-
Thermoregulation and risk of surgical site infection.Infect Control Hosp Epidemiol. 2011 Jun;32(6):603-10. doi: 10.1086/660017. Infect Control Hosp Epidemiol. 2011. PMID: 21558774 Review.
-
Selection pressures of vancomycin powder use in spine surgery: a meta-analysis.Spine J. 2019 Jun;19(6):1076-1084. doi: 10.1016/j.spinee.2019.01.002. Epub 2019 Jan 17. Spine J. 2019. PMID: 30660741
Cited by
-
Risk factors for surgical site infection following colorectal resection: a multi-institutional study.Int J Colorectal Dis. 2016 Feb;31(2):267-71. doi: 10.1007/s00384-015-2413-5. Epub 2015 Oct 28. Int J Colorectal Dis. 2016. PMID: 26507963
-
Time Trends and Predictors of Abnormal Postoperative Body Temperature in Infants Transported to the Intensive Care Unit.Anesthesiol Res Pract. 2016;2016:7318137. doi: 10.1155/2016/7318137. Epub 2016 Sep 29. Anesthesiol Res Pract. 2016. PMID: 27777585 Free PMC article.
-
Unintended perioperative hypothermia.Ochsner J. 2011 Fall;11(3):259-70. Ochsner J. 2011. PMID: 21960760 Free PMC article.
-
Guidelines for Perioperative Care for Liver Surgery: Enhanced Recovery After Surgery (ERAS) Society Recommendations.World J Surg. 2016 Oct;40(10):2425-40. doi: 10.1007/s00268-016-3700-1. World J Surg. 2016. PMID: 27549599
-
Association Between Perioperative Hypothermia and Surgical Site Infection After Elective Abdominal Surgery: A Prospective Cohort Study.Cureus. 2020 Oct 25;12(10):e11145. doi: 10.7759/cureus.11145. Cureus. 2020. PMID: 33251055 Free PMC article.
References
-
- National Nosocomial Infections Surveillance (NNIS) system report, data summary from January 1992–June 2001, issued August 2001. Am J Infect Control. 2001;29:404–421. - PubMed
-
- Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and economic outcomes attributable to methicillin resistance among patients with Staphylococcus aureus surgical site infection. Clin Infect Dis. 2003;36:592–598. - PubMed
-
- Kirkland KB, Briggs JP, Trivette SL, et al. The impact of surgical-site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect Control Hosp Epidemiol. 1999;20:725–730. - PubMed
-
- Dimick JB, Chen SL, Taheri PA, et al. Hospital costs associated with surgical complications: a report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531–537. - PubMed
-
- Scott R. The Direct Medical Costs of Healthcare-Associated Infections in US Hospitals and the Benefits of Prevention. Available at: http://www.cdc.gov/ncidod/dhqp/pdf/Scott_CostPaper.pdf. Cited March 26, 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
