

Change in vascular access and hospitalization risk in long-term hemodialysis patients
- PMID: 20884778
- PMCID: PMC3001775
- DOI: 10.2215/CJN.08961209
Change in vascular access and hospitalization risk in long-term hemodialysis patients
Abstract
Background and objectives: Conversion from central venous catheters to a graft or a fistula is associated with lower mortality risk in long-term hemodialysis (HD) patients; however, a similar association with hospitalization risk remains to be elucidated.
Design, setting, participants, & measurements: We conducted a prospective observational study all maintenance in-center HD patients who were treated in Fresenius Medical Care, North America legacy facilities; were alive on January 1, 2007; and had baseline laboratory data from December 2006. Access conversion (particularly from a catheter to a fistula or a graft) during the 4-month period from January 1 through April 30, 2007, was linked using Cox models to hospitalization risk during the succeeding 1-year follow-up period (until April 30, 2008).
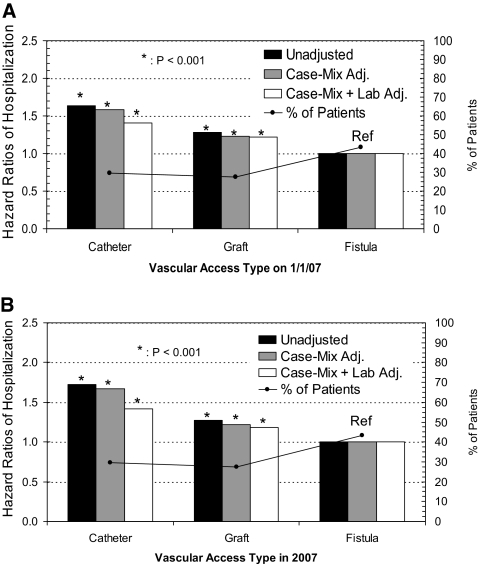
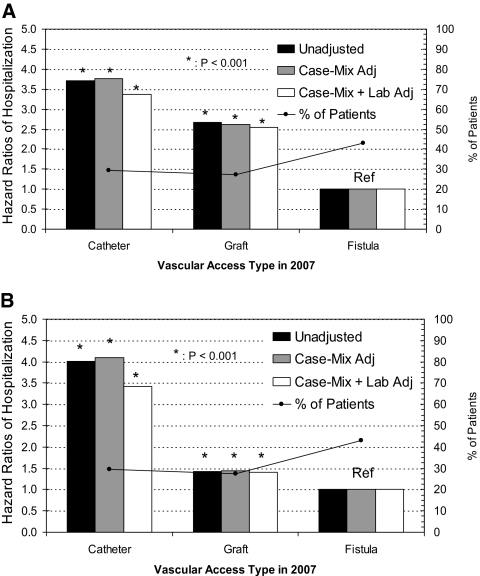
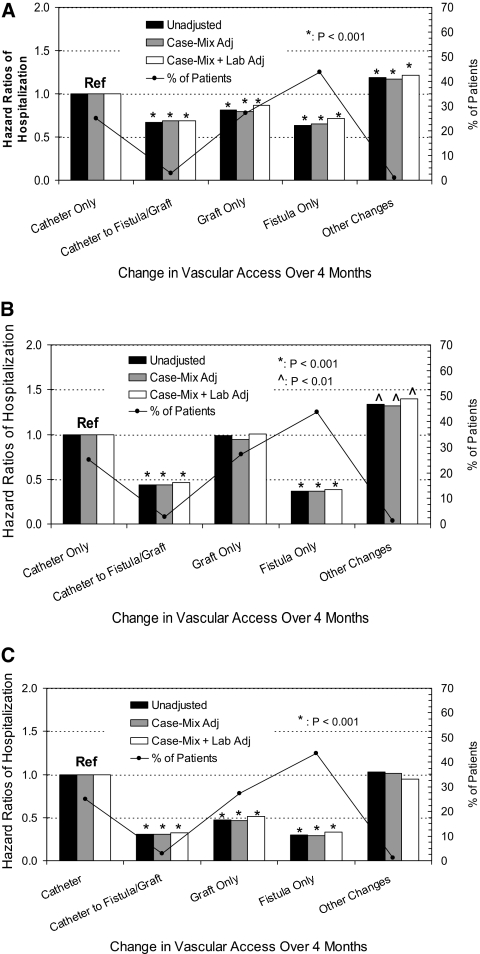
Results: The cohort (N = 79,545) on January 1, 2007 had 43% fistulas, 29% catheters, and 27% grafts. By April 30, 2007, 70,852 patients were still on HD, and among 19,792 catheters initially, only 10.3% (2045 patients) converted to either a graft or a fistula. With catheters as reference, patients who converted to grafts/fistulas had similar adjusted hazard ratios (0.69) as patients on fistulas (0.71), while patients with fistulas/grafts who converted to catheters did worse (1.22), all P < 0.0001.
Conclusions: Catheters remain associated with the greatest hospitalization risk. Conversion from a catheter to either graft or fistula had significantly lower hospitalization risk relative to keeping the catheter. Prospective studies are needed to determine whether programs that reduce catheters will decrease hospitalization risk in HD patients.
Figures
References
-
- NKF-DOQI clinical practice guidelines for vascular access. National Kidney Foundation-Dialysis Outcomes Quality Initiative. Am J Kidney Dis 30: S150–S191, 1997 - PubMed
-
- III. NKF-K/DOQI clinical practice guidelines for vascular access: Update 2000. Am J Kidney Dis 37: S137–S181, 2001 - PubMed
-
- National Kidney Foundation: KDOQI clinical practice guidelines and clinical practice recommendations: 2006 updates—Vascular access. Am J Kidney Dis 48: S176–S307, 2006 - PubMed
-
- Lacson E, Jr, Lazarus JM, Himmelfarb J, Ikizler TA, Hakim RM: Balancing Fistula First with Catheters Last. Am J Kidney Dis 50: 379–395, 2007 - PubMed
-
- Lok CE: Fistula first initiative: Advantages and pitfalls. Clin J Am Soc Nephrol 2: 1043–1053, 2007 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
