

Surgical outcomes for older patients with glioblastoma multiforme: preoperative factors associated with decreased survival. Clinical article
- PMID: 20887095
- PMCID: PMC4020429
- DOI: 10.3171/2010.8.JNS1081
Surgical outcomes for older patients with glioblastoma multiforme: preoperative factors associated with decreased survival. Clinical article
Abstract
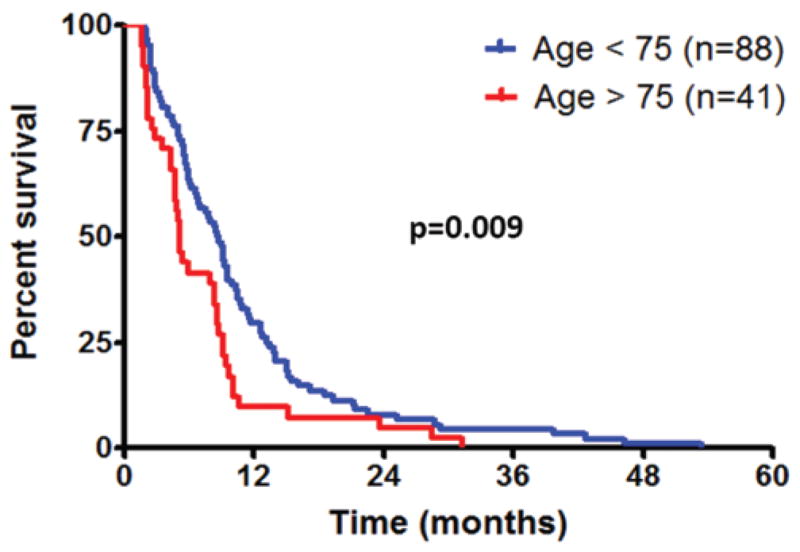
Object: As the population ages, the incidence of glioblastoma multiforme (GBM) among older patients (age > 65 years) will increase. Older patients, unlike their younger counterparts, are not often offered aggressive surgery because of their age, comorbidities, and potential inability to tolerate surgery. The goal of this study was to identify preoperative factors associated with decreased survival for older patients who underwent resection of a GBM. The identification of these factors may provide insight into which patients would benefit most from aggressive surgery.
Methods: All patients older than 65 years who underwent nonbiopsy resection of an intracranial GBM at a single institution between 1997 and 2007 were retrospectively reviewed. Factors associated with overall survival were assessed using multivariate proportional hazards regression analysis after controlling for peri- and postoperative factors known to be associated with outcome (extent of resection, carmustine wafer implantation, temozolomide chemotherapy, and radiation therapy). Variables with p < 0.05 were considered statistically significant.
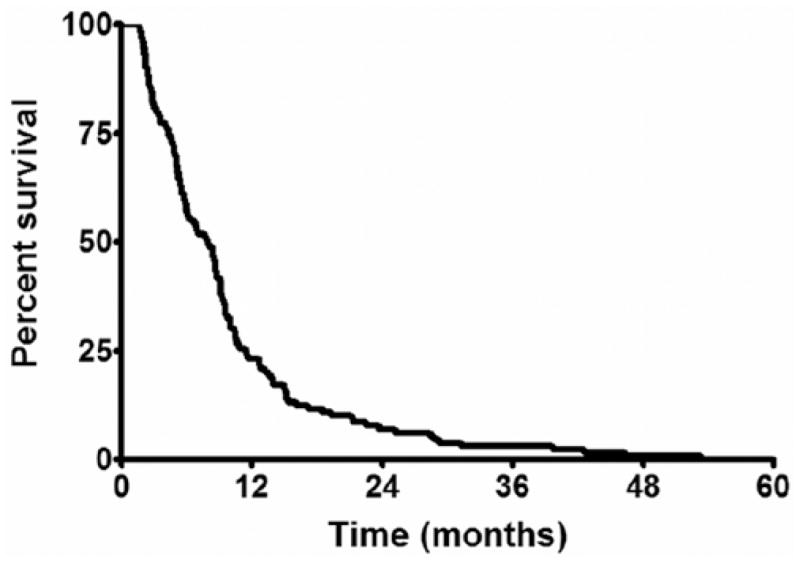
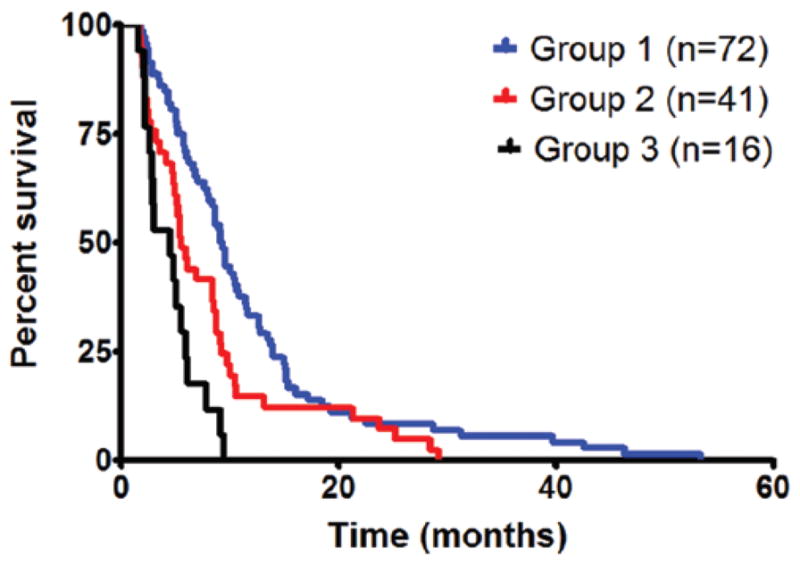
Results: A total of 129 patients with an average age of 73 ± 5 years met the inclusion/exclusion criteria. At last follow-up, all 129 patients had died, with a median survival of 7.9 months. The preoperative factors that were independently associated with decreased survival were Karnofsky Performance Scale (KPS) score less than 80 (p = 0.001), chronic obstructive pulmonary disease (p = 0.01), motor deficit (p = 0.01), language deficit (p = 0.005), cognitive deficit (p = 0.02), and tumor size larger than 4 cm (p = 0.002). Patients with 0-1 (Group 1), 2-3 (Group 2), and 4-6 (Group 3) of these factors had statistically different survival times, where the median survival was 9.2, 5.5, and 4.4 months, respectively. In log-rank analysis, the median survival for Group 1 was significantly longer than that for Group 2 (p = 0.004) and Group 3 (p < 0.0001), while Group 2 had longer survival than Group 3 (p = 0.02).
Conclusions: Older patients with an increasing number of these factors may not benefit as much from aggressive surgery as patients with fewer factors. This may provide insight into identifying which patients older than 65 years of age may benefit from aggressive surgery.
Conflict of interest statement
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Author contributions to the study and manuscript preparation include the following. Conception and design: KL Chaichana. Acquisition of data: KL Chaichana, KK Chaichana. Analysis and interpretation of data: Quiñones-Hinojosa, KL Chaichana, Olivi, Weingart. Drafting the article: KL Chaichana, KK Chaichana, Olivi, Bennett, Brem. Critically revising the article: Quiñones-Hinojosa, KL Chaichana, Olivi, Weingart, Bennett, Brem. Reviewed final version of the manuscript and approved it for submission: all authors. Statistical analysis: KL Chaichana. Administrative/technical/material support: Quiñones-Hinojosa, KL Chaichana. Study supervision: Quiñones-Hinojosa, KL Chaichana.
Figures
Comment in
-
Surgery for glioblastoma multiforme.J Neurosurg. 2011 Mar;114(3):585-6; discussion 586. doi: 10.3171/2010.8.JNS101143. Epub 2010 Oct 1. J Neurosurg. 2011. PMID: 20887086 No abstract available.
-
Glioblastoma in the elderly.J Neurosurg. 2012 Feb;116(2):355-6; discussion 356. doi: 10.3171/2011.6.JNS11982. Epub 2011 Sep 23. J Neurosurg. 2012. PMID: 21942728 No abstract available.
References
-
- Alonso M, Hamelin R, Kim M, Porwancher K, Sung T, Parhar P, et al. Microsatellite instability occurs in distinct subtypes of pediatric but not adult central nervous system tumors. Cancer Res. 2001;61:2124–2128. - PubMed
-
- Barnholtz-Sloan JS, Maldonado JL, Williams VL, Curry WT, Rodkey EA, Barker FG, II, et al. Racial/ethnic differences in survival among elderly patients with a primary glioblastoma. J Neurooncol. 2007;85:171–180. - PubMed
-
- Brandes AA, Compostella A, Blatt V, Tosoni A. Glioblastoma in the elderly: current and future trends. Crit Rev Oncol Hematol. 2006;60:256–266. - PubMed
-
- Brandes AA, Franceschi E, Tosoni A, Benevento F, Scopece L, Mazzocchi V, et al. Temozolomide concomitant and adjuvant to radiotherapy in elderly patients with glioblastoma: correlation with MGMT promoter methylation status. Cancer. 2009;115:3512–3518. - PubMed
-
- Brem H, Piantadosi S, Burger PC, Walker M, Selker R, Vick NA, et al. Placebo-controlled trial of safety and efficacy of intraoperative controlled delivery by biodegradable polymers of chemotherapy for recurrent gliomas. Lancet. 1995;345:1008–1012. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
