

The bridge stent technique for salvage of pancreaticojejunal anastomotic dehiscence
- PMID: 20887326
- PMCID: PMC2997664
- DOI: 10.1111/j.1477-2574.2010.00227.x
The bridge stent technique for salvage of pancreaticojejunal anastomotic dehiscence
Abstract
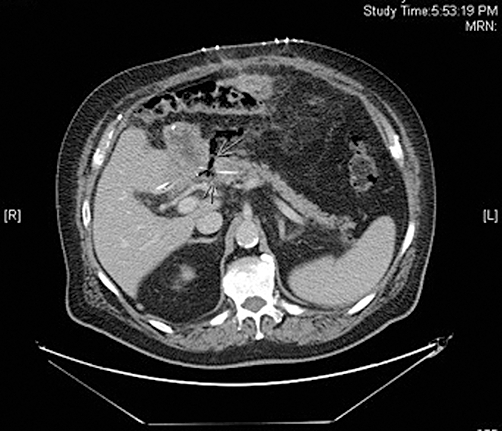
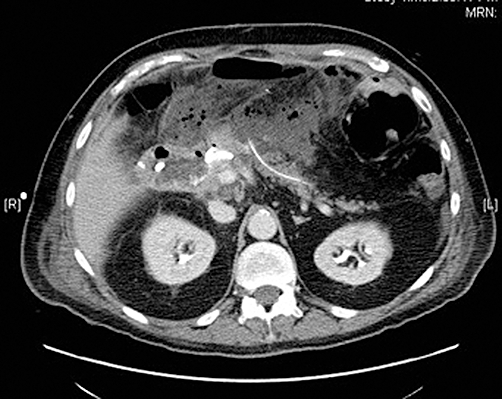
Objectives: Although infrequent, Grade C postoperative pancreatic fistulae (POPF) following pancreaticoduodenectomy (PD) are morbid and potentially lethal. Traditional management of a disrupted pancreaticojejunostomy (PJ) anastomosis consists of either wide external drainage or completion pancreatectomy. The aim of this study is to describe an alternative management approach to PJ dehiscence after PD.
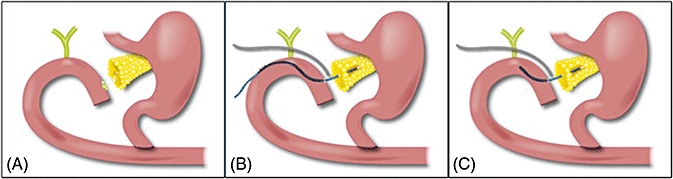
Methods: A bridge stent technique is employed in the setting of a disrupted PJ anastomosis. Upon re-exploration, a 5-Fr or 8-Fr silastic feeding tube stent is placed across a gap between the jejunal enterotomy and the pancreatic duct, and secured with an absorbable suture at both ends. Depending upon the degree of local inflammation, this may be externalized by coursing the stent downstream through the pancreaticobiliary drainage limb in a Witzel fashion.
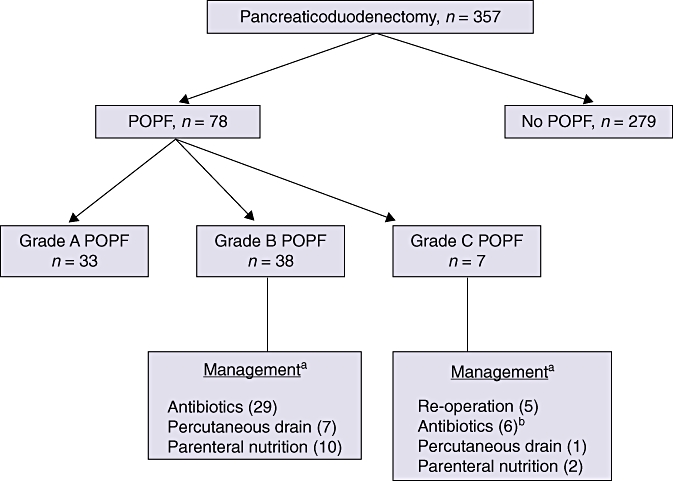
Results: Over 8 years and 357 PDs with duct-to-mucosa PJ reconstruction, seven ISGPF (International Study Group on Pancreatic Fistula) Grade C fistulae occurred (2%). Two patients ultimately died secondary to POPF (neither anastomosis was dehisced). The described technique was used in the other five patients, all of whom had evidence of a dehisced PJ anastomosis. All originally had at least two or three recognized risk factors for POPF development (high-risk pathology, soft gland, duct diameter ≤ 3 mm, estimated blood loss ≥ 1000 ml). All patients survived this complication and were discharged from hospital. There have been no longterm external fistulae, nor any recognized PJ strictures or remnant atrophy (median follow-up: 10.7 months).
Conclusions: In the context of a dehisced pancreaticojejunal anastomosis, the bridge stent technique is a safe and effective method of management that contributes to diminished mortality and helps to salvage pancreatic function.
© 2010 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery. 2005;138:8–13. - PubMed
-
- Guéroult S, Parc Y, Duron F, Paye F, Parc R. Completion pancreatectomy for postoperative peritonitis after pancreaticoduodenectomy. Arch Surg. 2004;139:16–19. - PubMed
-
- van Berge Henegouwen MI, De Wit LT, van Gulik TM, Obertop H, Gouma DJ. Incidence, risk factors, and treatment of pancreatic leakage after pancreaticoduodenectomy: drainage versus resection of the pancreatic remnant. J Am Coll Surg. 1997;185:18–24. - PubMed
-
- Farley DR, Schwall G, Trede M. Completion pancreatectomy for surgical complications after pancreaticoduodenectomy. Br J Surg. 1996;83:176–179. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
