

Advanced systems to assess colonoscopy
- PMID: 20889073
- PMCID: PMC10602402
- DOI: 10.1016/j.giec.2010.07.012
Advanced systems to assess colonoscopy
Abstract
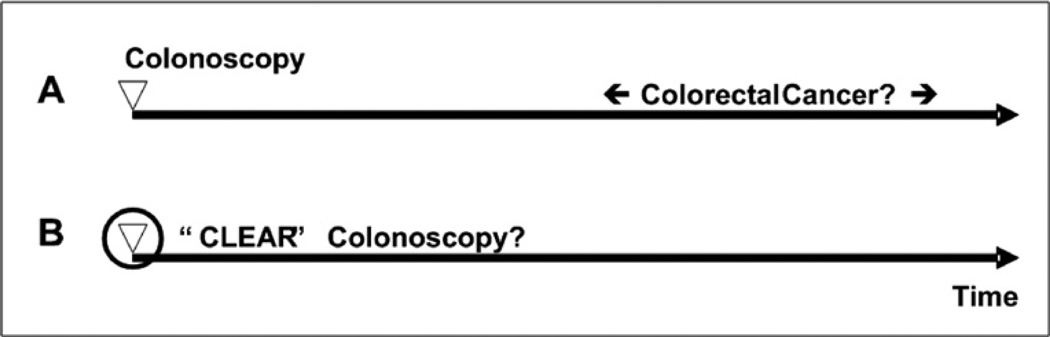
Colorectal cancer is the second major cause of cancer-related death in the United States. The long time involved in progression of mucosal dysplasia from a small polyp to an invasive cancer and the ability to image the colon mucosa are features that make early detection and prevention of colorectal cancer by colonoscopy possible. Although colonoscopy has contributed to a marked decline in the number of colorectal cancer-related deaths, the protective effect of colonoscopy, when used in routine clinical practice, has not lived up to the expectations raised by carefully controlled prospective research studies. Therefore new systems that assess quality of colonoscopy are needed.
Copyright © 2010. Published by Elsevier Inc.
Figures
References
-
- Jemal A, Siegel R, Ward E, et al. Cancer statistics2009. CA Cancer J Clin. 2009;59(4):225–249. - PubMed
-
- Bressler B, Paszat LF, Chen Z, et al. Rates of new or missed colorectal cancers after colonoscopy and their risk factors: a population-based analysis. Gastroenterology. 2007;132(1):96–102. - PubMed
-
- Johnson CD, Fletcher JG, MacCarty RL, et al. Effect of slice thickness and primary 2D versus 3D virtual dissection on colorectal lesion detection at CT colonography in 452 asymptomatic adults. AJR Am J Roentgenol. 2007;189(3):672–680. - PubMed
-
- Baxter NN, Goldwasser MA, Paszat LF, et al. Association of colonoscopy and death from colorectal cancer. Ann Intern Med. 2009;150(1):1. - PubMed
-
- Hewett DG, Kahi CJ, Rex DK. Does colonoscopy work? J Natl Compr Canc Netw. 2010;8(1):67–77. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
