

Cost-effectiveness of colonoscopy
- PMID: 20889076
- PMCID: PMC4145837
- DOI: 10.1016/j.giec.2010.07.008
Cost-effectiveness of colonoscopy
Abstract
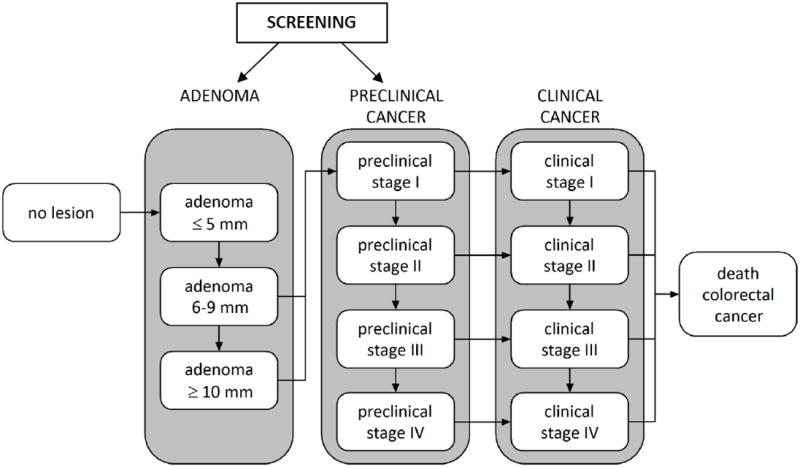
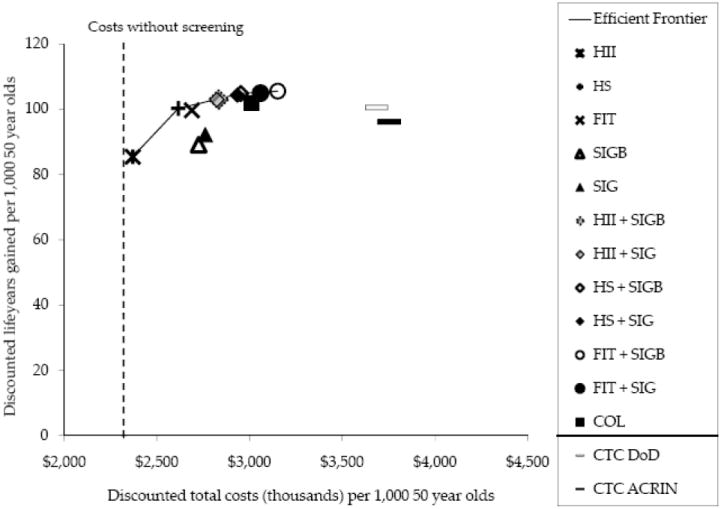
This article presents a cost-effectiveness analysis of colorectal cancer screening tests that have been recommended by the United States Preventive Services Task Force, American Cancer Society US Multi-Society Task Force on Colorectal Cancer American College of Radiology, or the American College of Gastroenterology. This cost-effectiveness analysis supports a common theme of the 3 guideline groups that there are multiple acceptable colorectal cancer screening strategies (including colonoscopy). The article shows which recommended strategies are also cost-effective given a range of willingness to pay per life-year gained. The set of cost-effective strategies includes tests that primarily detect cancer early (annual sensitive fecal occult blood tests [FOBTs]; either guaiac or fecal immunochemical tests, but not Hemoccult II), as well as those that can prevent colorectal cancer (flexible sigmoidoscopy every 5 years with a frequent sensitive FOBT [but not flexible sigmoidoscopy as a standalone test], and colonoscopy). Computed tomographic colonography was not a cost-effective strategy. Stool DNA testing was not assessed in the analysis for this article.
Copyright © 2010 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancer screening: clinical guidelines and rationale. Gastroenterology. 1997 Feb;112(2):594–642. - PubMed
-
- Mandel J, Bond J, Church T, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood. Minnesota Colon Cancer Control Study. N Engl J Med. 1993 May 13;328(19):1365–1371. - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MH, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996 Nov 30;348(9040):1472–1477. - PubMed
-
- Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sondergaard O. Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet. 1996 Nov 30;348(9040):1467–1471. - PubMed
-
- Selby JV, Friedman GD, Quesenberry CP, Jr, Weiss NS. A case-control study of screening sigmoidoscopy and mortality from colorectal cancer. N Engl J Med. 1992 Mar 5;326(10):653–657. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
