

The pathogenesis of primary cicatricial alopecias
- PMID: 20889564
- PMCID: PMC2966773
- DOI: 10.2353/ajpath.2010.100454
The pathogenesis of primary cicatricial alopecias
Abstract
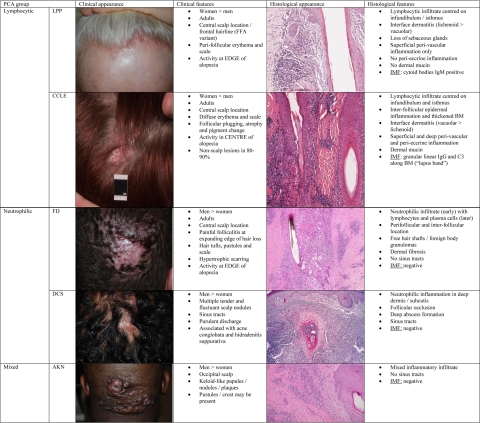
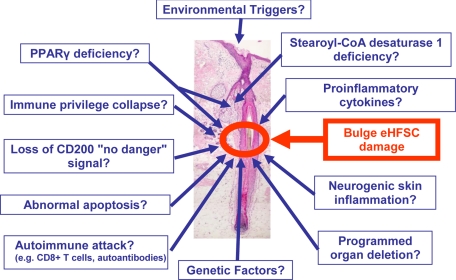
Cicatricial (scarring) alopecia results from irreversible damage to epithelial stem cells located in the bulge region of the hair follicle, generally as a result of inflammatory mechanisms (eg, in the context of autoimmune disease). In primary cicactricial alopecia (PCA), the hair follicle itself is the key target of autoaggressive immunity. This group of permanent hair loss disorders can be classified into distinct subgroups, characterized by the predominant peri-follicular inflammatory cell type. In none of these PCA forms do we know exactly why hair follicles begin to attract such an infiltrate. Thus, it is not surprising that halting or even reversing this inflammation in PCA is often extremely difficult. However, increasing evidence suggests that healthy hair follicle epithelial stem cells enjoy relative protection from inflammatory assault by being located in an immunologically "privileged" niche. Because this protection may collapse in PCA, one key challenge in PCA research is to identify the specific signaling pathways that endanger, or restore, the relative immunoprotection of these stem cells. After a summary of pathobiological principles that underlie the development and clinical phenotype of PCA, we close by defining key open questions that need to be answered if more effective treatment modalities for this therapeutically very frustrating, but biologically fascinating, group of diseases are to be developed.
Figures
References
-
- Harries MJ, Trueb RM, Tosti A, Messenger AG, Chaudhry I, Whiting DA, Sinclair R, Griffiths CE, Paus R. How not to get scar(r) ed: pointers to the correct diagnosis in patients with suspected primary cicatricial alopecia. Br J Dermatol. 2009;160:482–501. - PubMed
-
- Whiting DA. Cicatricial alopecia: clinico-pathological findings and treatment. Clin Dermatol. 2001;19:211–225. - PubMed
-
- Tiede S, Kloepper JE, Bodo E, Tiwari S, Kruse C, Paus R. Hair follicle stem cells: walking the maze. Eur J Cell Biol. 2007;86:355–376. - PubMed
-
- Mecklenburg L, Tobin DJ, Muller-Rover S, Handjiski B, Wendt G, Peters EM, Pohl S, Moll I, Paus R. Active hair growth (anagen) is associated with angiogenesis. J Invest Dermatol. 2000;114:909–916. - PubMed
-
- Botchkarev VA, Botchkareva NV, Peters EM, Paus R. Epithelial growth control by neurotrophins: leads and lessons from the hair follicle. Prog Brain Res. 2004;146:493–513. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
