

Periodic assessment of plasma sFlt-1 and PlGF concentrations and its association with placental morphometry in gestational hypertension (GH) - a prospective follow-up study
- PMID: 20920154
- PMCID: PMC2958153
- DOI: 10.1186/1471-2393-10-58
Periodic assessment of plasma sFlt-1 and PlGF concentrations and its association with placental morphometry in gestational hypertension (GH) - a prospective follow-up study
Abstract
Background: Hypertensive disorders in pregnancy contributes to about 12% of maternal deaths in Malaysia and similarly worldwide. Early detection and adequate management are preventable strategies. Biochemical markers of abnormal angiogenesis would be more specific in early detection than routine blood pressure and proteinuria measurements. The aim of this study was to estimate maternal plasma PlGF and sFlt-1 levels in pregnant women with gestational hypertension at three intervals of pregnancy and correlate these biomarker levels with placental morphometry.
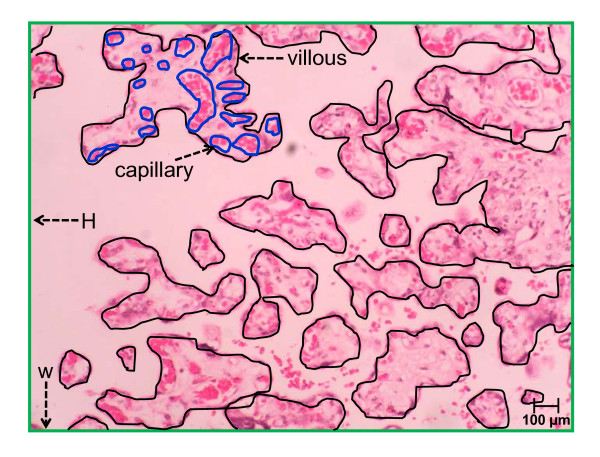
Methods: Venous blood samples (antepartum, intrapartum and post partum periods) were drawn to estimate for sFlt-1 and PlGF levels while placental tissue samples were examined for placental morphometry.
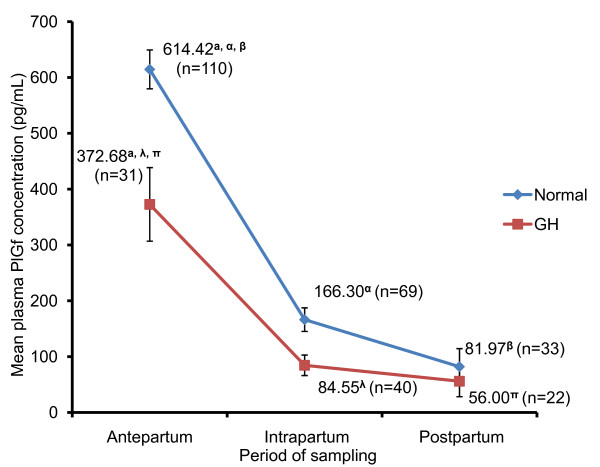
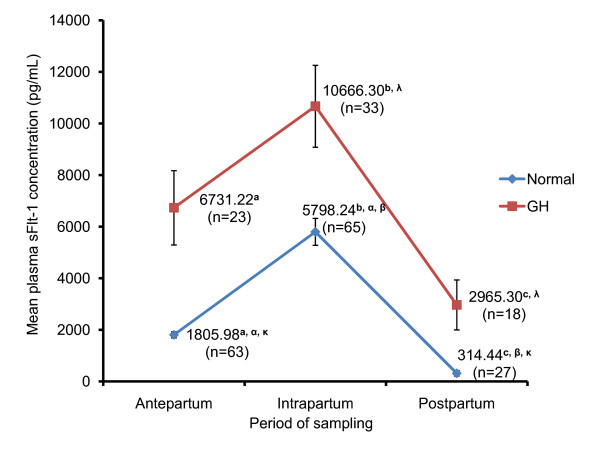
Results: PlGF levels were lower in gestational hypertension (GH) compared to normotensive during antepartum and intrapartum period, whereas sFlt-1 levels were elevated in GH at antepartum, intrapartum and postpartum intervals during pregnancy. An inverse relationship between these two biomarkers was observed through correlation analysis. PlGF levels were inversely correlated with total villous surface area of the placental periphery (TCsa-C) and villous capillarization (VC-C) of the placental periphery.
Conclusion: We established periodic values of for sFlt-1 and PlGF levels for the first time in an ethnically diverse Malaysian setting. We suggest the development of GH in women is related to defective capillarization. In demonstrating periodic changes, this study suggest the possibility of developing GH and other long term health complications as a result of prolonged exposure to sFlt-1. The correlation between PlGF levels and morphometric findings also support possible capillarization defect.
Figures
References
-
- Managing Eclampsia - Educational Material For Teachers Of Midwifery. http://whqlibdoc.who.int/publications/2008/9789241546669_2_eng.pdf
-
- Malaysia MoH. Report on Confidential Enquiries into Maternal Deaths 1997-2000, Ministry of Health Malaysia
-
- Zhou Y, McMaster M, Woo K, Janatpour M, Perry J, Karpanen T, Alitalo K, Damsky C, Fisher SJ. Vascular endothelial growth factor ligands and receptors that regulate human cytotrophoblast survival are dysregulated in severe preeclampsia and hemolysis, elevated liver enzymes, and low platelets syndrome. Am J Pathol. 2002;160(4):1405–1423. - PMC - PubMed
-
- Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, Libermann TA, Morgan JP, Sellke FW, Stillman IE. et al. Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia. J Clin Invest. 2003;111(5):649–658. - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
