

On-ward participation of a hospital pharmacist in a Dutch intensive care unit reduces prescribing errors and related patient harm: an intervention study
- PMID: 20920322
- PMCID: PMC3219276
- DOI: 10.1186/cc9278
On-ward participation of a hospital pharmacist in a Dutch intensive care unit reduces prescribing errors and related patient harm: an intervention study
Abstract
Introduction: Patients admitted to an intensive care unit (ICU) are at high risk for prescribing errors and related adverse drug events (ADEs). An effective intervention to decrease this risk, based on studies conducted mainly in North America, is on-ward participation of a clinical pharmacist in an ICU team. As the Dutch Healthcare System is organized differently and the on-ward role of hospital pharmacists in Dutch ICU teams is not well established, we conducted an intervention study to investigate whether participation of a hospital pharmacist can also be an effective approach in reducing prescribing errors and related patient harm (preventable ADEs) in this specific setting.
Methods: A prospective study compared a baseline period with an intervention period. During the intervention period, an ICU hospital pharmacist reviewed medication orders for patients admitted to the ICU, noted issues related to prescribing, formulated recommendations and discussed those during patient review meetings with the attending ICU physicians. Prescribing issues were scored as prescribing errors when consensus was reached between the ICU hospital pharmacist and ICU physicians.
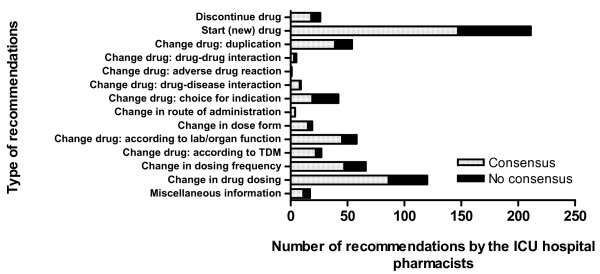
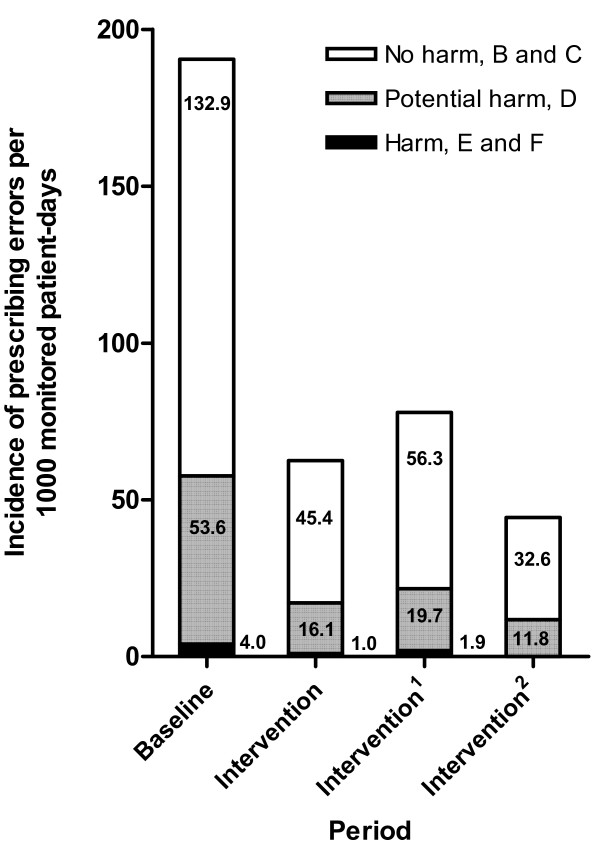
Results: During the 8.5-month study period, medication orders for 1,173 patients were reviewed. The ICU hospital pharmacist made a total of 659 recommendations. During the intervention period, the rate of consensus between the ICU hospital pharmacist and ICU physicians was 74%. The incidence of prescribing errors during the intervention period was significantly lower than during the baseline period: 62.5 per 1,000 monitored patient-days versus 190.5 per 1,000 monitored patient-days, respectively (P < 0.001). Preventable ADEs (patient harm, National Coordinating Council for Medication Error Reporting and Prevention severity categories E and F) were reduced from 4.0 per 1,000 monitored patient-days during the baseline period to 1.0 per 1,000 monitored patient-days during the intervention period (P = 0.25). Per monitored patient-day, the intervention itself cost €3, but might have saved €26 to €40 by preventing ADEs.
Conclusions: On-ward participation of a hospital pharmacist in a Dutch ICU was associated with significant reductions in prescribing errors and related patient harm (preventable ADEs) at acceptable costs per monitored patient-day.
Trial registration number: ISRCTN92487665.
Figures
Comment in
-
Minimising drug errors in critically ill patients.Crit Care. 2011 Jan 11;15(1):401; author reply 401. doi: 10.1186/cc9366. Crit Care. 2011. PMID: 21235830 Free PMC article. No abstract available.
References
-
- Kohn LT, Corrigan JM, Donaldson MS, editors. To Err is Human: Building a Safer Health System. Washington DC: National Academy Press; 2000. - PubMed
-
- Zegers M, de Bruijne MC, Wagner C, Hoonhout LH, Waaijman R, Smits M, Hout FA, Zwaan L, Christiaans-Dingelhoff I, Timmermans DR, Groenewegen PP, van der Wal G. Adverse events and potentially preventable deaths in Dutch hospitals: results of a retrospective patient record review study. Qual Saf Health Care. 2009;18:297–302. doi: 10.1136/qshc.2007.025924. - DOI - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
