

Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa
- PMID: 20921118
- PMCID: PMC3038846
- DOI: 10.1001/archgenpsychiatry.2010.128
Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa
Abstract
Context: Evidence-based treatment trials for adolescents with anorexia nervosa are few.
Objective: To evaluate the relative efficacy of family-based treatment (FBT) and adolescent-focused individual therapy (AFT) for adolescents with anorexia nervosa in full remission.
Design: Randomized controlled trial.
Setting: Stanford University and The University of Chicago (April 2005 until March 2009).
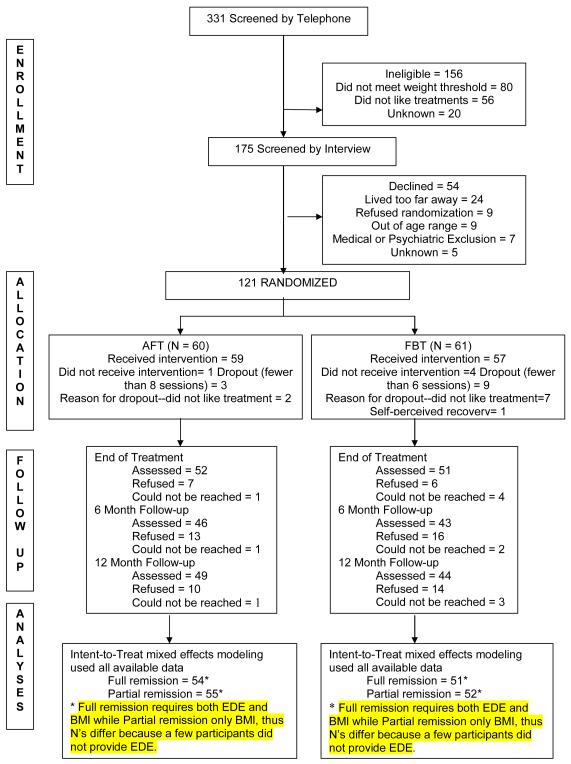
Participants: One hundred twenty-one participants, aged 12 through 18 years, with DSM-IV diagnosis of anorexia nervosa excluding the amenorrhea requirement. Intervention Twenty-four outpatient hours of treatment over 12 months of FBT or AFT. Participants were assessed at baseline, end of treatment (EOT), and 6 months' and 12 months' follow-up posttreatment.
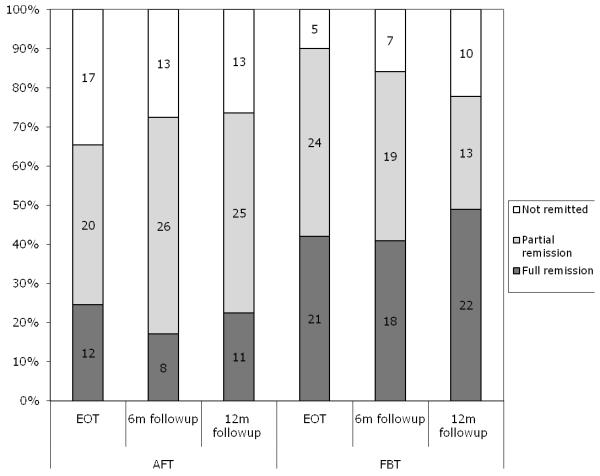
Main outcome measures: Full remission from anorexia nervosa defined as normal weight (≥95% of expected for sex, age, and height) and mean global Eating Disorder Examination score within 1 SD of published means. Secondary outcome measures included partial remission rates (>85% of expected weight for height plus those who were in full remission) and changes in body mass index percentile and eating-related psychopathology.
Results: There were no differences in full remission between treatments at EOT. However, at both the 6- and 12-month follow-up, FBT was significantly superior to AFT on this measure. Family-based treatment was significantly superior for partial remission at EOT but not at follow-up. In addition, body mass index percentile at EOT was significantly superior for FBT, but this effect was not found at follow-up. Participants in FBT also had greater changes in Eating Disorder Examination score at EOT than those in AFT, but there were no differences at follow-up.
Conclusion: Although both treatments led to considerable improvement and were similarly effective in producing full remission at EOT, FBT was more effective in facilitating full remission at both follow-up points.
Trial registration: clinicaltrials.gov Identifier: NCT00149786.
Figures
Comment in
-
Family-based treatment increases full remission at 1-year follow-up compared with adolescent-focused individual therapy in adolescents with anorexia nervosa.Evid Based Ment Health. 2011 Feb;14(1):27. doi: 10.1136/ebmh.14.1.27. Evid Based Ment Health. 2011. PMID: 21266624 No abstract available.
References
-
- Hoek H. Review of epidemiological studies of eating disorders. Int Rev Psychiatry. 1993;5:61–74.
-
- Hoek H, Hoeken Dv. Review of prevalence and incidence of eating disorders. Int J Eat Disord. 2003;34:383–396. - PubMed
-
- Hoek H, van Harten PN, Hermans KM, et al. The incidence of anorexia nervosa on Curacao. Am J. Psychiatry. 2005;162:748–752. - PubMed
-
- van Son G, van hoeken D, Aad I, et al. Time trends in the incidence of eating disorders: a primary care study in the Netherlands. Int J Eat Disord. 2006;39:565–569. - PubMed
-
- Rome E, Ammerman S. Medical complications of eating disorders: An update. Journal of Adolecent Health. 2003;33:418–426. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
