

Review
doi: 10.1136/gut.2009.206250.
Epub 2010 Oct 4.
Colorectal cancer molecular biology moves into clinical practice
Affiliations
- PMID: 20921207
- PMCID: PMC3006043
- DOI: 10.1136/gut.2009.206250
Item in Clipboard
Review
Colorectal cancer molecular biology moves into clinical practice
Gut.
2011 Jan.
Abstract
The promise of personalised medicine is now a clinical reality, with colorectal cancer genetics at the forefront of this next major advance in clinical medicine. This is no more evident than in the recent advances in testing of colorectal cancers for specific molecular alterations in order to guide treatment with the monoclonal antibody therapies cetuximab and panitumumab, which target the epidermal growth factor receptor. In this review, genetic mechanisms of colorectal cancer and how these alterations relate to emerging biomarkers for early detection and risk stratification (diagnostic markers), prognosis (prognostic markers) and the prediction of treatment responses (predictive markers) are examined.
Figures
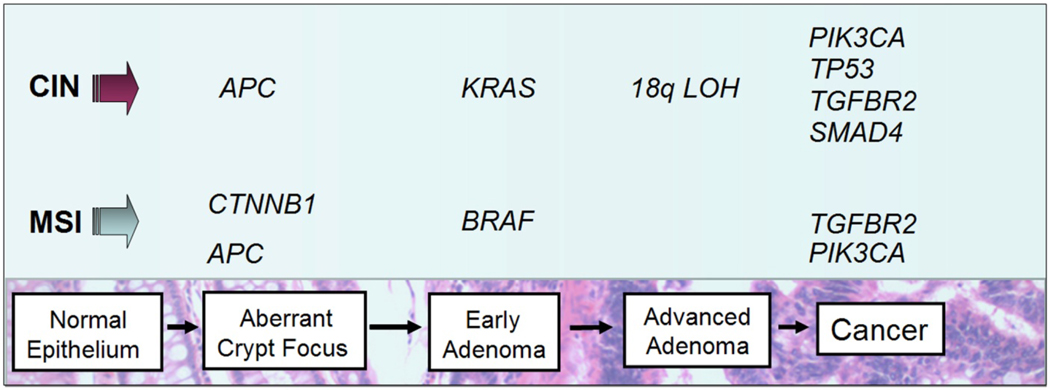
Colorectal carcinogenesis progresses by at least two well-recognized pathways. The chromosome instability (CIN) pathway is characterized by classic tubular adenoma histology and the early acquisition of APC mutations that lead to deregulated WNT signaling, frequent activating mutations of the KRAS oncogene at the early adenoma stage, loss of heterozygosity at chromosome 18q (18qLOH) in late adenomas, and TP53 mutations that facilitate the transition to frank malignancy. By contrast, tumors that harbor microsatellite instability (MSI) frequently acquire BRAF mutations and are not associated with 18qLOH or TP53 mutations. Sporadic MSI cancers appear to commonly arise via the serrated neoplasia pathway, in which sessile serrated adenomas are the most frequently observed pre-cancerous lesions.
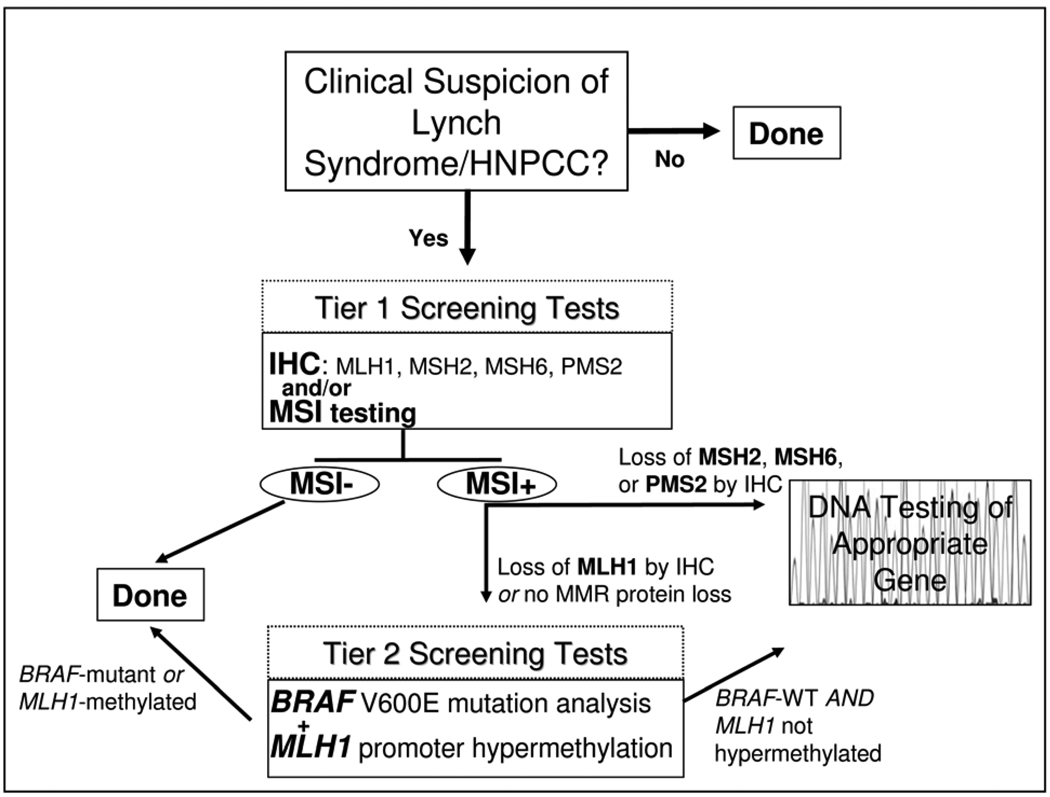
A multi-stage approach to facilitate the cost-effective diagnosis of Lynch Syndrome is outlined. Patients with a high clinical suspicion of Lynch Syndrome are first screened by immunohistochemistry (IHC) studies of the tumor tissue to assess for loss of Mismatch Repair proteins (MMR) expression and by MSI testing of the tumor DNA (Tier 1 Screening Tests). Patients with tumors that show microsatellite instability (MSI) with loss of MSH2, MSH6, or PMS2 by IHC undergo germline DNA mutation analysis of the gene corresponding to the missing protein. In contrast, patients with MSI tumors that lack MLH1 are further assessed with assessment of the tumor for MLH1 promoter methylation and mutant BRAF V600E (Tier 2 Screening Test) because most sporadic MSI colon cancers have methylated MLH1 and Lynch Syndrome MSI cancers rarely harbor BRAF mutations. When there is not evidence of MLH1 promoter methylation or BRAF mutation, mutation analysis of the MLH1 gene is performed to identify Lynch Syndrome patients with mutations in this gene.
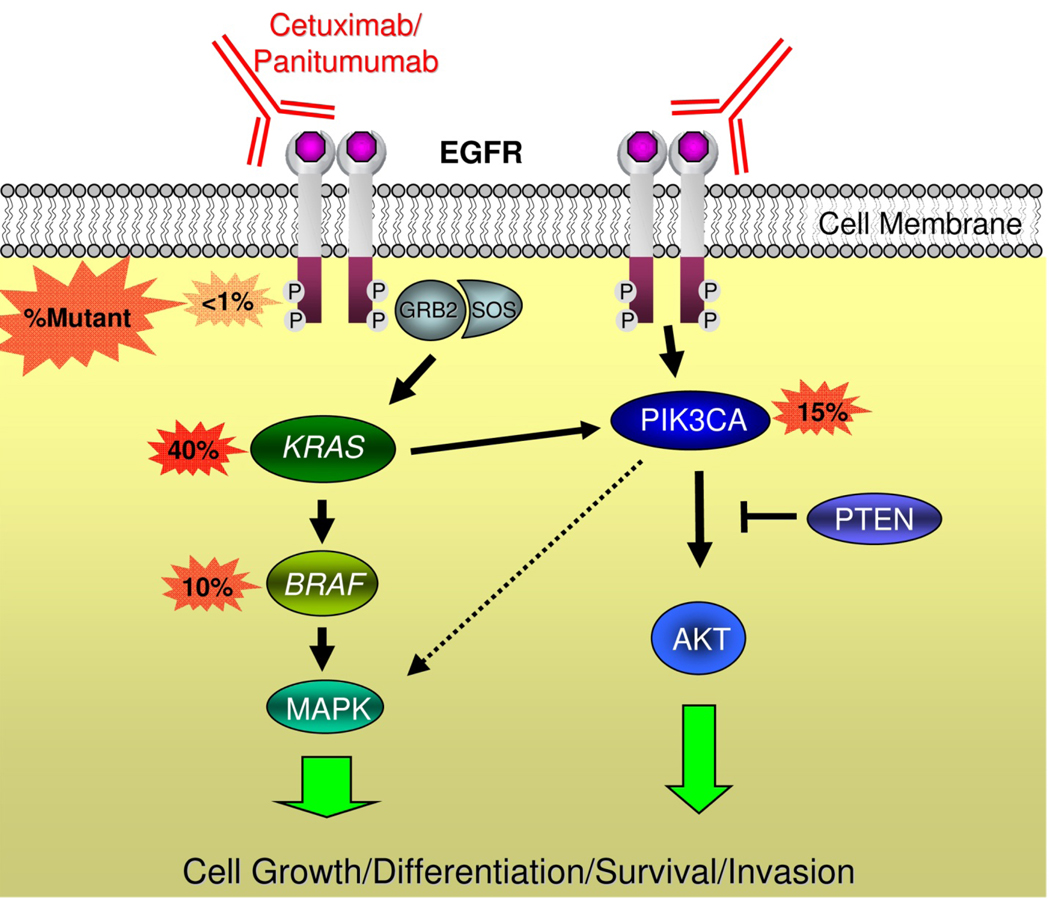
EGFR forms a homodimer after ligand activation, which results in phosphorylation/activation of the intra-cellular kinase domain and a cascade of downstream signaling including activation of the Ras/Raf/MAPK and phosphoinositol-3-kinase (PI3K) pathways that are associated with cell growth, differentiation, survival, and invasion. Monoclonal antibodies used to treat patients with metastatic colorectal cancer including cetuximab and panitumumab bind to the extracellular portion of EGFR and inhibit signaling in some patients. Activating mutations in KRAS occur in ~40% of colorectal cancers and are thought to confer resistance to these drugs by bypassing the need for upstream EGFR signals. Activating mutations in BRAF – the direct downstream effector of KRAS – occur in ~10% of colorectal cancers and also probably confer resistance to anti-EGFR monoclonal antibodies. Emerging evidence supports an additional role of oncogenic aberrations in the PI3K pathway in cetuximab and panitumumab resistance.
References
-
- European Medicines Agency. Committee for Medicinal Products for Human Use May 2008 Plenary Meeting monthly report. 2008. http://www.emea.europa.eu/pdfs/human/press/pr/27923508en.pdf.
-
- National Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in Oncology: Colon Cancer V.2.2010. 2010. http://www.nccn.org/professionals/physician_gls/PDF/colon.pdf. - PubMed
-
- Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH, Hayes DF, et al. American Society of Clinical Oncology provisional clinical opinion: testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J Clin Oncol. 2009;27:2091–2096. - PubMed
-
- Karapetis CS, Khambata-Ford S, Jonker DJ, O'Callaghan CJ, Tu D, Tebbutt NC, et al. K-ras mutations and benefit from cetuximab in advanced colorectal cancer. N Engl J Med. 2008;359:1757–1765. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials