Management of infrabony defects in mandibular molars in a patient with generalized aggressive periodontitis using autogenous bone graft from maxillary tuberosity
- PMID: 20922081
- PMCID: PMC2933531
- DOI: 10.4103/0972-124X.65443
Management of infrabony defects in mandibular molars in a patient with generalized aggressive periodontitis using autogenous bone graft from maxillary tuberosity
Abstract
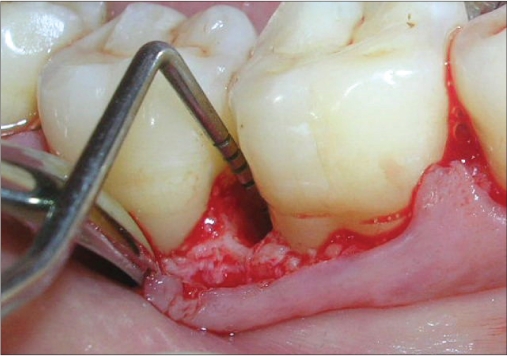
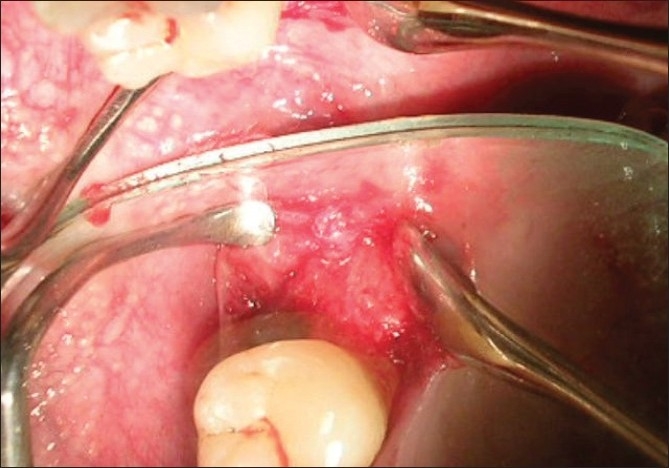
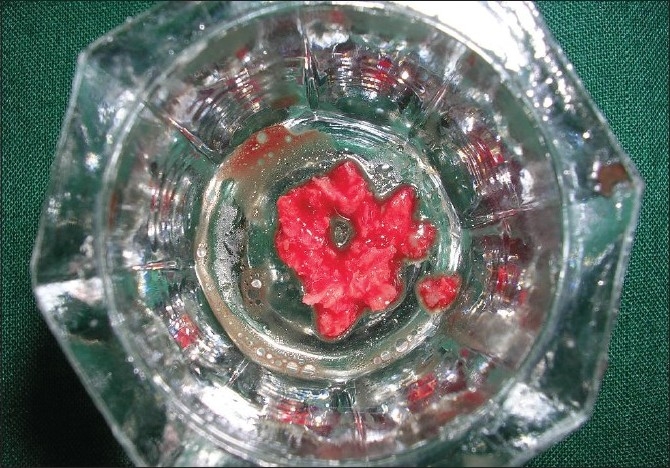
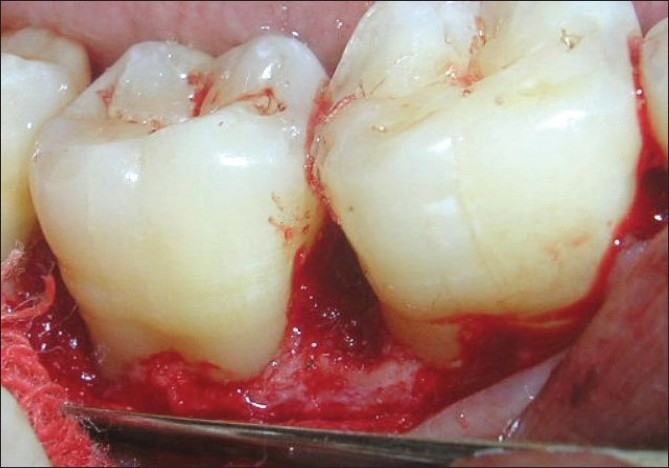
This clinical case report presents a technique utilizing autogenous cancellous bone from maxillary tuberosity to fill two infrabony defects distal to mandibular molars in a patient diagnosed with aggressive periodontitis. After debridement a 6 mm defect was present distal to mandibular right first molar and 6.5 mm defect was present distal to mandibular second molar of same side. Autogenous bone graft from maxillary tuberosity was placed in both the defects. There was a significant bony fill present six months post surgery and probing depth reduced by 7mm on both the sites.
Keywords: Autogenous bone graft; generalized aggressive periodontitis; infrabony defect.
Conflict of interest statement
Figures








References
-
- Garrett S. Periodontal regeneration around natural teeth. Ann Periodontol. 1996;1:621–70. - PubMed
-
- Ramjford SP, Caffesse RG, Morrison EC, Hill RW, Kerry GJ, Appleberry EA, et al. Four modalities of periodontal treatment compared over 5 years. J Clin Periodontol. 1987;14:445–52. - PubMed
-
- Reynolds M, Aichelmann-Reidy W, Branch Mays G. The efficacy of bone replacement grafts in the treatment of periodontal osseous defects: A sytematic review. Ann Periodontol. 2003;1:227–65. - PubMed
-
- Dragoo MR, Sullivan HC. A clinical and histological evaluation of autogenous iliac bone grafts in humans I: Wound healing 2 to 8 months. J Periodontol. 1973;44:599–613. - PubMed
-
- Froum SJ, Ortiz M, Witkin RT, Thaler R, Scopp IW, Stahl SS. Osseous autografts III: Comparison of osseous coagulum-bone blend implants with open curettage. J Periodontol. 1976;47:287–94. - PubMed