

Comparison of two active case-finding strategies for community-based diagnosis of symptomatic smear-positive tuberculosis and control of infectious tuberculosis in Harare, Zimbabwe (DETECTB): a cluster-randomised trial
- PMID: 20923715
- PMCID: PMC2956882
- DOI: 10.1016/S0140-6736(10)61425-0
Comparison of two active case-finding strategies for community-based diagnosis of symptomatic smear-positive tuberculosis and control of infectious tuberculosis in Harare, Zimbabwe (DETECTB): a cluster-randomised trial
Abstract
Background: Control of tuberculosis in settings with high HIV prevalence is a pressing public health priority. We tested two active case-finding strategies to target long periods of infectiousness before diagnosis, which is typical of HIV-negative tuberculosis and is a key driver of transmission.
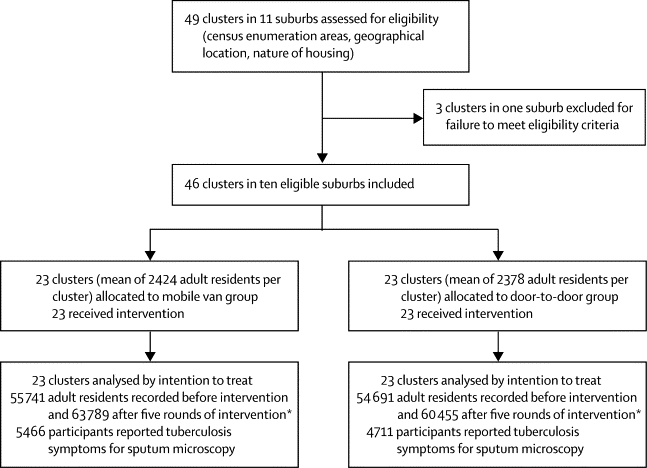
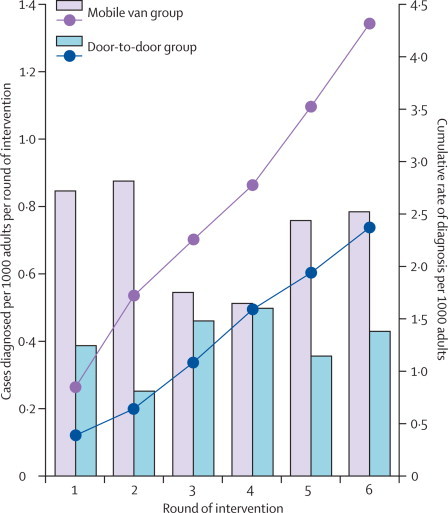
Methods: Clusters of neighbourhoods in the high-density residential suburbs of Harare, Zimbabwe, were randomised to receive six rounds of active case finding at 6-monthly intervals by either mobile van or door-to-door visits. Randomisation was done by selection of discs of two colours from an opaque bag, with one disc to represent every cluster, and one colour allocated to each intervention group before selection began. In both groups, adult (≥16 years) residents volunteering chronic cough (≥2 weeks) had two sputum specimens collected for fluorescence microscopy. Community health workers and cluster residents were not masked to intervention allocation, but investigators and laboratory staff were masked to allocation until final analysis. The primary outcome was the cumulative yield of smear-positive tuberculosis per 1000 adult residents, compared between intervention groups; analysis was by intention to treat. The secondary outcome was change in prevalence of culture-positive tuberculosis from before intervention to before round six of intervention in 12% of randomly selected households from the two intervention groups combined; analysis was based on participants who provided sputum in the two prevalence surveys. This trial is registered, number ISRCTN84352452.
Findings: 46 study clusters were identified and randomly allocated equally between intervention groups, with 55 741 adults in the mobile van group and 54,691 in the door-to-door group at baseline. HIV prevalence was 21% (1916/9060) and in the 6 months before intervention the smear-positive case notification rate was 2·8 per 1000 adults per year. The trial was completed as planned with no adverse events. The mobile van detected 255 smear-positive patients from 5466 participants submitting sputum compared with 137 of 4711 participants identified through door-to-door visits (adjusted risk ratio 1·48, 95% CI 1·11-1·96, p=0·0087). The overall prevalence of culture-positive tuberculosis declined from 6·5 per 1000 adults (95% CI 5·1-8·3) to 3·7 per 1000 adults (2·6-5·0; adjusted risk ratio 0·59, 95% CI 0·40-0·89, p=0·0112).
Interpretation: Wide implementation of active case finding, particularly with a mobile van approach, could have rapid effects on tuberculosis transmission and disease.
Funding: Wellcome Trust.
Copyright © 2010 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Active case-finding for TB in the community: time to act.Lancet. 2010 Oct 9;376(9748):1205-6. doi: 10.1016/S0140-6736(10)61503-6. Lancet. 2010. PMID: 20923714 No abstract available.
References
-
- WHO . Global tuberculosis control: epidemiology, strategy, financing. WHO/HTM/TB/2009.411. World Health Organization; Geneva: 2009.
-
- Glynn JR, Crampin AC, Yates MD. The importance of recent infection with Mycobacterium tuberculosis in an area with high HIV prevalence: a long-term molecular epidemiological study in northern Malawi. J Infect Dis. 2005;192:480–487. - PubMed
-
- Verver S, Warren RM, Munch Z. Proportion of tuberculosis transmission that takes place in households in a high-incidence area. Lancet. 2004;363:212–214. - PubMed
-
- Corbett EL, Marston B, Churchyard GJ, De Cock KM. Tuberculosis in sub-Saharan Africa: opportunities, challenges and change in the era of antiretroviral treatment. Lancet. 2006;367:926–937. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
