

Out-of-hospital hypertonic resuscitation following severe traumatic brain injury: a randomized controlled trial
- PMID: 20924011
- PMCID: PMC3015143
- DOI: 10.1001/jama.2010.1405
Out-of-hospital hypertonic resuscitation following severe traumatic brain injury: a randomized controlled trial
Abstract
Context: Hypertonic fluids restore cerebral perfusion with reduced cerebral edema and modulate inflammatory response to reduce subsequent neuronal injury and thus have potential benefit in resuscitation of patients with traumatic brain injury (TBI).
Objective: To determine whether out-of-hospital administration of hypertonic fluids improves neurologic outcome following severe TBI.
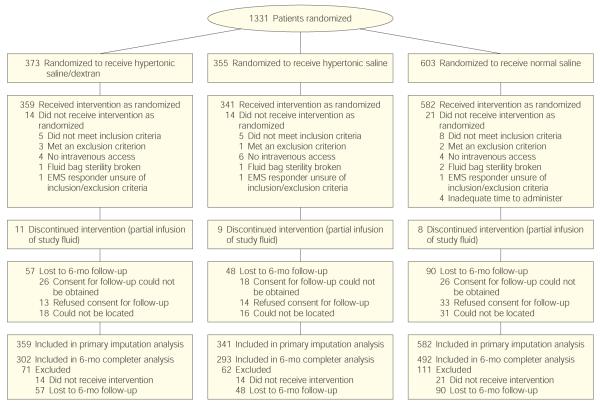
Design, setting, and participants: Multicenter, double-blind, randomized, placebo-controlled clinical trial involving 114 North American emergency medical services agencies within the Resuscitation Outcomes Consortium, conducted between May 2006 and May 2009 among patients 15 years or older with blunt trauma and a prehospital Glasgow Coma Scale score of 8 or less who did not meet criteria for hypovolemic shock. Planned enrollment was 2122 patients.
Intervention: A single 250-mL bolus of 7.5% saline/6% dextran 70 (hypertonic saline/dextran), 7.5% saline (hypertonic saline), or 0.9% saline (normal saline) initiated in the out-of-hospital setting.
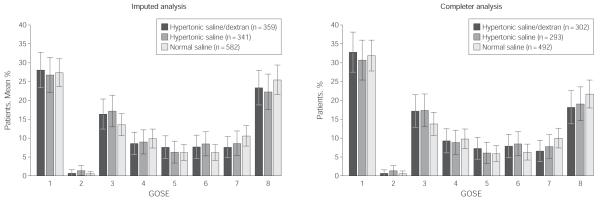
Main outcome measure: Six-month neurologic outcome based on the Extended Glasgow Outcome Scale (GOSE) (dichotomized as >4 or ≤4).
Results: The study was terminated by the data and safety monitoring board after randomization of 1331 patients, having met prespecified futility criteria. Among the 1282 patients enrolled, 6-month outcomes data were available for 1087 (85%). Baseline characteristics of the groups were equivalent. There was no difference in 6-month neurologic outcome among groups with regard to proportions of patients with severe TBI (GOSE ≤4) (hypertonic saline/dextran vs normal saline: 53.7% vs 51.5%; difference, 2.2% [95% CI, -4.5% to 9.0%]; hypertonic saline vs normal saline: 54.3% vs 51.5%; difference, 2.9% [95% CI, -4.0% to 9.7%]; P = .67). There were no statistically significant differences in distribution of GOSE category or Disability Rating Score by treatment group. Survival at 28 days was 74.3% with hypertonic saline/dextran, 75.7% with hypertonic saline, and 75.1% with normal saline (P = .88).
Conclusion: Among patients with severe TBI not in hypovolemic shock, initial resuscitation with either hypertonic saline or hypertonic saline/dextran, compared with normal saline, did not result in superior 6-month neurologic outcome or survival.
Trial registration: clinicaltrials.gov Identifier: NCT00316004.
Figures
References
-
- Gross CP, Anderson GF, Powe NR. The relation between funding by the National Institutes of Health and the burden of disease. N Engl J Med. 1999;340(24):1881–1887. - PubMed
-
- Sell SL, Avila MA, Yu G, et al. Hypertonic resuscitation improves neuronal and behavioral outcomes after traumatic brain injury plus hemorrhage. Anesthesiology. 2008;108(5):873–881. - PubMed
-
- Tyagi R, Donaldson K, Loftus CM, Jallo J. Hypertonic saline: a clinical review. Neurosurg Rev. 2007;30(4):277–290. - PubMed
-
- Rockswold GL, Solid CA, Paredes-Andrade E, Rockswold SB, Jancik JT, Quickel RR. Hypertonic saline and its effect on intracranial pressure, cerebral perfusion pressure, and brain tissue oxygen. Neurosurgery. 2009;65(6):1035–1042. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- HL077873/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- UL1 TR000005/TR/NCATS NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- U01 HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
- HL077865/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
