

Simultaneously anterior decompression and posterior instrumentation by extrapleural retroperitoneal approach in thoracolumbar lesions
- PMID: 20924482
- PMCID: PMC2947728
- DOI: 10.4103/0019-5413.69315
Simultaneously anterior decompression and posterior instrumentation by extrapleural retroperitoneal approach in thoracolumbar lesions
Abstract
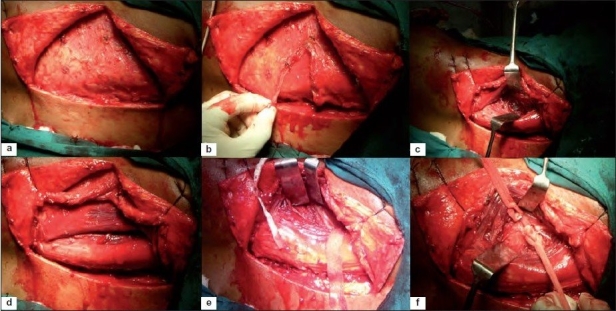
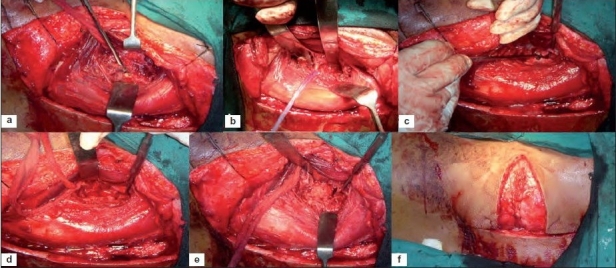
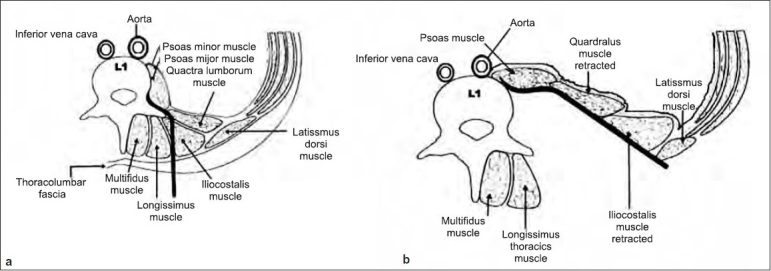
Background: Anterior decompression with posterior instrumentation when indicated in thoracolumbar spinal lesions if performed simultaneously in single-stage expedites rehabilitation and recovery. Transthoracic, transdiaphragmatic approach to access the thoracolumbar junction is associated with significant morbidity, as it violates thoracic cavity; requires cutting of diaphragm and a separate approach, for posterior instrumentation. We evaluated the clinical outcome morbidity and feasibility of extrapleural retroperitoneal approach to perform anterior decompression and posterior instrumentation simultaneously by single "T" incision outcome in thoracolumbar spinal trauma and tuberculosis.
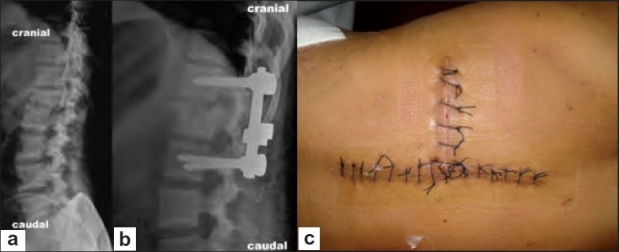
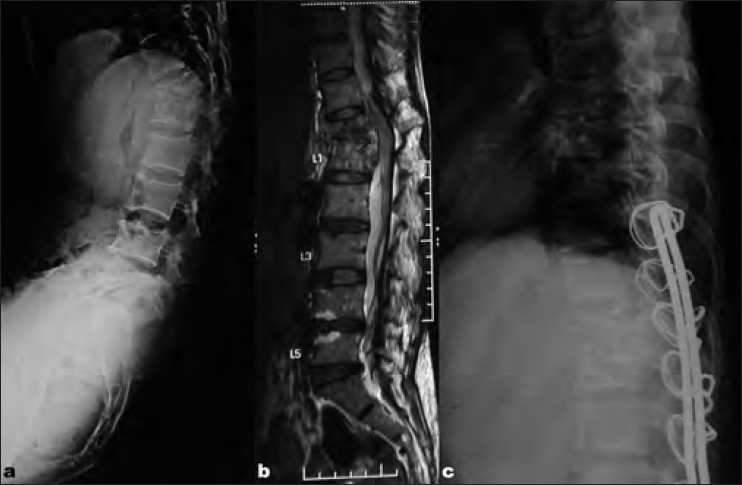
Patients and methods: Forty-eight cases of tubercular spine (n = 25) and fracture of the spine (n = 23) were included in the study of which 29 were male and 19 female. The mean age of patients was 29.1 years. All patients underwent single-stage anterior decompression, fusion, and posterior instrumentation (except two old traumatic cases) via extrapleural retroperitoneal approach by single "T" incision. Tuberculosis cases were operated in lateral position as they were stabilized with Hartshill instrumentation. For traumatic spine initially posterior pedicle screw fixation was performed in prone position and then turned to right lateral position for anterior decompression by same incision and approach. They were evaluated for blood loss, duration of surgery, superficial and deep infection of incision site, flap necrosis, correction of the kyphotic deformity, and restoration of anterior and posterior vertebral body height.
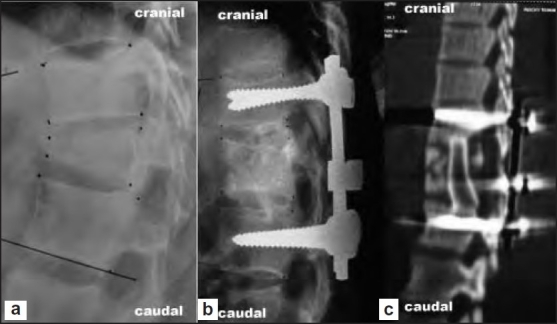
Results: In traumatic spine group the mean duration of surgery was 269 minutes (range 215-315 minutes) including the change over time from prone to lateral position. The mean intraoperative blood loss was 918 ml (range 550-1100 ml). The preoperative mean ASIA motor, pin prick and light touch score improved from 63.3 to 74.4, 86 to 94.4 and 86 to 96 at 6 month of follow-up respectively. The mean preoperative loss of the anterior vertebral height improved from 44.7% to 18.4% immediate postoperatively and was 17.5% at final follow-up at 1 year. The means preoperative kyphus angle also improved from 23.3° to 9.3° immediately after surgery, which deteriorated to 11.5° at final follow-up. One patient developed deep wound infection at the operative site as well as flap necrosis, which needed debridement and removal of hardware. Five patients had bed sore in the sacral region, which healed uneventfully. In tubercular spine (n=25) group, mean operating time was approximately 45 minutes less than traumatic group. The mean intraoperative blood loss was 1100 ml (750-2200 ml). The mean preoperative kyphosis was corrected from 55° to 23°. Wound healing occurred uneventful in 23 cases and wound dehiscence occurred in only 2 cases. Nine out of 11 cases with paraplegia showed excellent neural recovery while 2 with panvertebral disease showed partial neural recovery. None of the patients in both groups required intensive unit care.
Conclusions: Simultaneous exposure of both posterior and anterior column of the spine for posterior instrumentation and anterior decompression and fusion in single stage by extra pleural retroperitoneal approach by "T" incision in thoracolumbar spinal lesions is safe, an easy alternative with reduced morbidity as chest and abdominal cavities are not violated, ICU care is not required and diaphragm is not cut.
Keywords: Extra pleural retroperitoneal approach; spinal trauma; thoracolumbar spine; tuberculosis of spine.
Conflict of interest statement
Figures
References
-
- Papadopoulos SM, Fessler RG. Thoracic spine; anatomy and surgical approaches and exposures of the vertebral column. 2nd edi EC Benzel’s Spine Surgery; techniques, complications avoidance and management. Elsevier. 2005;1:281–93.
-
- Ikard RW. Methods and complications of anterior exposure of the thoracic and lumbar spine. Arch Surg. 2006;141:1025–34. - PubMed
-
- Jain AK, Dhammi IK, Prashad B, Sinha S, Mishra P. Simultaneous anterior decompression and posterior instrumentation of the tuberculous spine using an anterolateral extrapleural approach. J Bone Joint Surg. 2008;90:1477–81. - PubMed
-
- Jain AK, Maheshwari AV, Jain S. Kyphus correction in spinal tuberculosis. Clin Orthop Relat Res. 2007;460:117–23. - PubMed
-
- Jain AK, Agrrawal A, Dhammi IK, Aggrawal PK, Singh S. Extrapleural anterolateral decompression in tuberculosis of the dorsal spine. J Bone Joint Surg. 2004;86:1027–31. - PubMed
LinkOut - more resources
Full Text Sources