

X-linked lymphoproliferative disease due to SAP/SH2D1A deficiency: a multicenter study on the manifestations, management and outcome of the disease
- PMID: 20926771
- PMCID: PMC3374620
- DOI: 10.1182/blood-2010-06-284935
X-linked lymphoproliferative disease due to SAP/SH2D1A deficiency: a multicenter study on the manifestations, management and outcome of the disease
Erratum in
- Blood. 2011 Nov 3;118(18):5060. Pachlopnick-Schmid, Jana [corrected to Pachlopnik Schmid, Jana]
Abstract
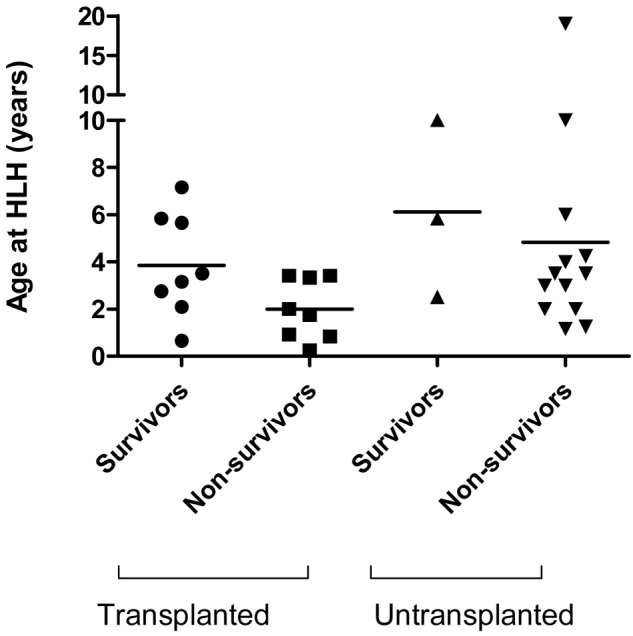
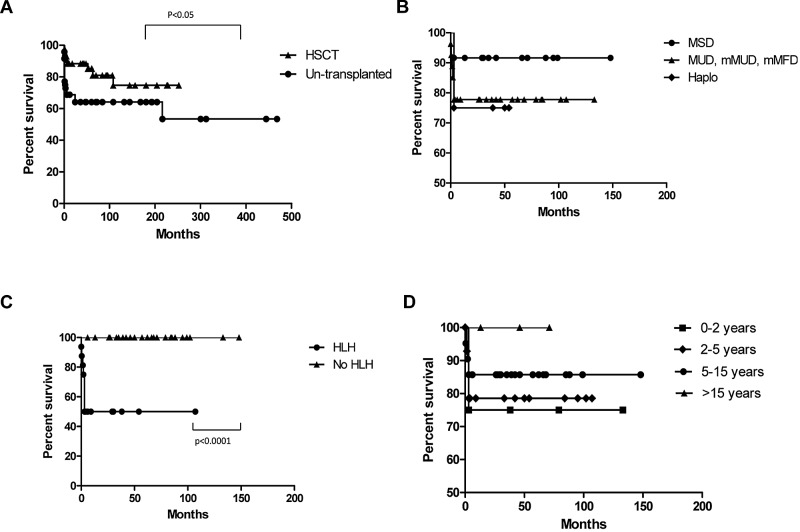
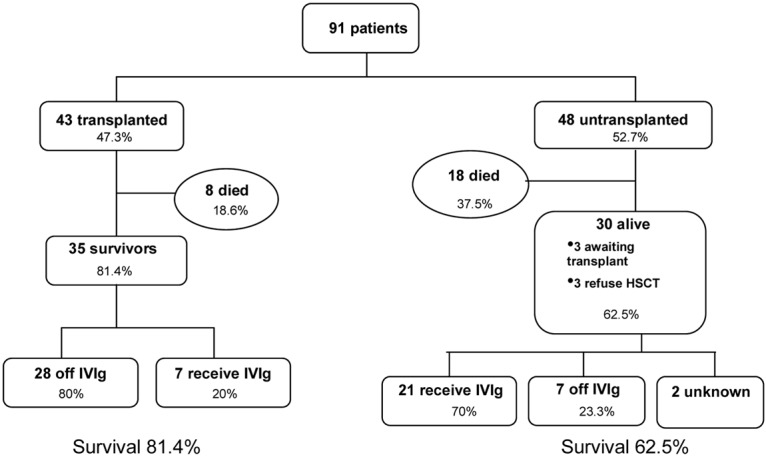
X-linked lymphoproliferative disease (XLP1) is a rare immunodeficiency characterized by severe immune dysregulation and caused by mutations in the SH2D1A/SAP gene. Clinical manifestations are varied and include hemophagocytic lymphohistiocytosis (HLH), lymphoma and dysgammaglobulinemia, often triggered by Epstein-Barr virus infection. Historical data published before improved treatment regimens shows very poor outcome. We describe a large cohort of 91 genetically defined XLP1 patients collected from centers worldwide and report characteristics and outcome data for 43 patients receiving hematopoietic stem cell transplant (HSCT) and 48 untransplanted patients. The advent of better treatment strategies for HLH and malignancy has greatly reduced mortality for these patients, but HLH still remains the most severe feature of XLP1. Survival after allogeneic HSCT is 81.4% with good immune reconstitution in the large majority of patients and little evidence of posttransplant lymphoproliferative disease. However, survival falls to 50% in patients with HLH as a feature of disease. Untransplanted patients have an overall survival of 62.5% with the majority on immunoglobulin replacement therapy, but the outcome for those untransplanted after HLH is extremely poor (18.8%). HSCT should be undertaken in all patients with HLH, because outcome without transplant is extremely poor. The outcome of HSCT for other manifestations of XLP1 is very good, and if HSCT is not undertaken immediately, patients must be monitored closely for evidence of disease progression.
Figures
References
-
- Purtilo DT, Cassel CK, Yang JP, Harper R. X-linked recessive progressive combined variable immunodeficiency (Duncan's disease). Lancet. 1975;1(7913):935–940. - PubMed
-
- Seemayer TA, Gross TG, Egeler RM, et al. X-linked lymphoproliferative disease: twenty-five years after the discovery. Pediatr Res. 1995;38(4):471–478. - PubMed
-
- Purtilo DT, Grierson HL. Methods of detection of new families with X-linked lymphoproliferative disease. Cancer Genet Cytogenet. 1991;51(2):143–153. - PubMed
-
- Sumegi J, Huang D, Lanyi A, et al. Correlation of mutations of the SH2D1A gene and Epstein-Barr virus infection with clinical phenotype and outcome in X-linked lymphoproliferative disease. Blood. 2000;96(9):3118–3125. - PubMed
-
- Rougemont AL, Fournet JC, Martin SR, et al. Chronic active gastritis in X-linked lymphoproliferative disease. Am J Surg Pathol. 2008;32(2):323–328. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
