

Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality
- PMID: 20927040
- PMCID: PMC3091945
- DOI: 10.1038/ki.2010.383
Rapid fluid removal during dialysis is associated with cardiovascular morbidity and mortality
Abstract
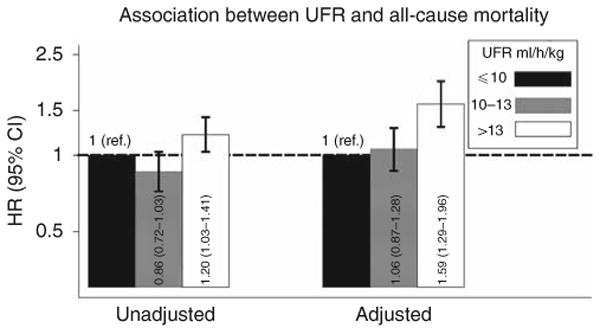
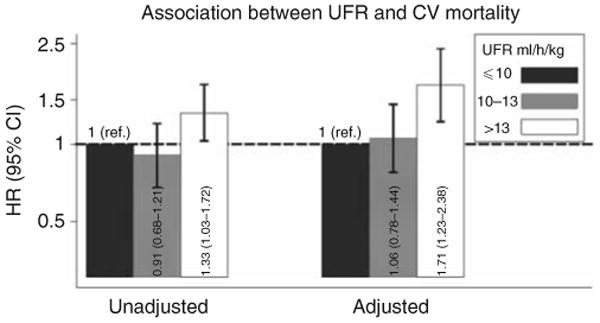
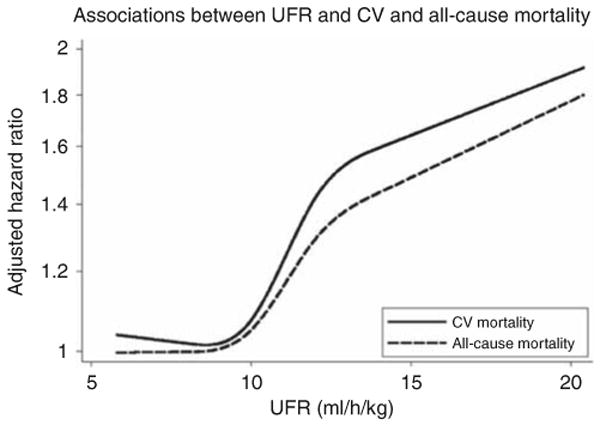
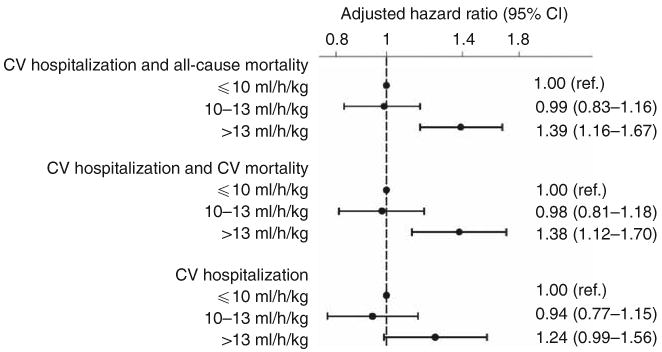
Patients receiving hemodialysis have high rates of cardiovascular morbidity and mortality that may be related to the hemodynamic effects of rapid ultrafiltration. Here we tested whether higher dialytic ultrafiltration rates are associated with greater all-cause and cardiovascular mortality, and hospitalization for cardiovascular disease. We used data from the Hemodialysis Study, an almost-7-year randomized clinical trial of 1846 patients receiving thrice-weekly chronic dialysis. The ultrafiltration rates were divided into three categories: up to 10 ml/h/kg, 10-13 ml/h/kg, and over 13 ml/h/kg. Compared to ultrafiltration rates in the lowest group, rates in the highest were significantly associated with increased all-cause and cardiovascular-related mortality with adjusted hazard ratios of 1.59 and 1.71, respectively. Overall, ultrafiltration rates between 10-13 ml/h/kg were not associated with all-cause or cardiovascular mortality; however, they were significantly associated among participants with congestive heart failure. Cubic spline interpolation suggested that the risk of all-cause and cardiovascular mortality began to increase at ultrafiltration rates over 10 ml/h/kg regardless of the status of congestive heart failure. Hence, higher ultrafiltration rates in hemodialysis patients are associated with a greater risk of all-cause and cardiovascular death.
Figures
Comment in
-
Rapid fluid removal and cardiovascular mortality.Nat Rev Nephrol. 2011 Jan;7(1):2. doi: 10.1038/nrneph.2010.164. Nat Rev Nephrol. 2011. PMID: 21218539 No abstract available.
References
-
- USRDS. Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; Bethesda, MD: 2008.
-
- Foley RN, Parfrey PS, Sarnak MJ. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am J Kidney Dis. 1998;32:S112–S119. - PubMed
-
- Weiner DE, Tighiouart H, Amin MG, et al. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15:1307–1315. - PubMed
-
- Shroff RC, McNair R, Figg N, et al. Dialysis accelerates medial vascular calcification in part by triggering smooth muscle cell apoptosis. Circulation. 2008;118:1748–1757. - PubMed
-
- Pecoits-Filho R, Heimburger O, Barany P, et al. Associations between circulating inflammatory markers and residual renal function in CRF patients. Am J Kidney Dis. 2003;41:1212–1218. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
