

Hair evaluation methods: merits and demerits
- PMID: 20927232
- PMCID: PMC2938572
- DOI: 10.4103/0974-7753.58553
Hair evaluation methods: merits and demerits
Abstract
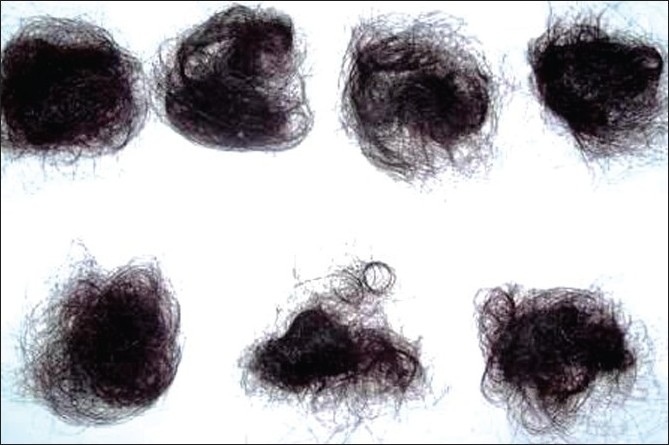
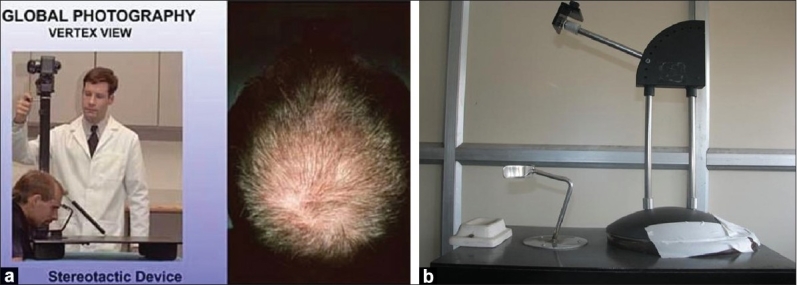
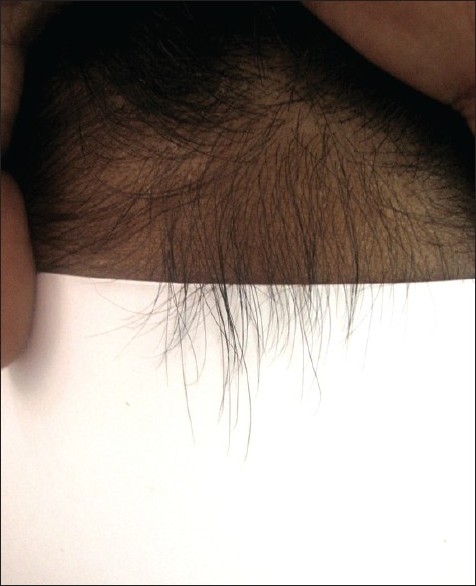
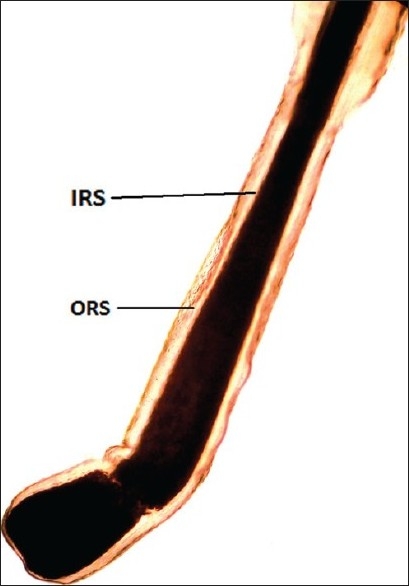
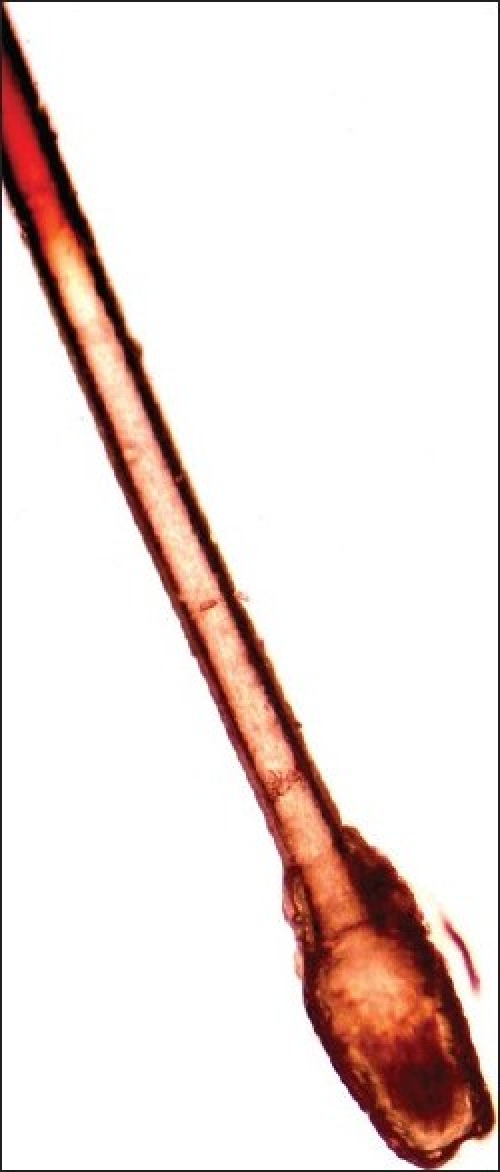
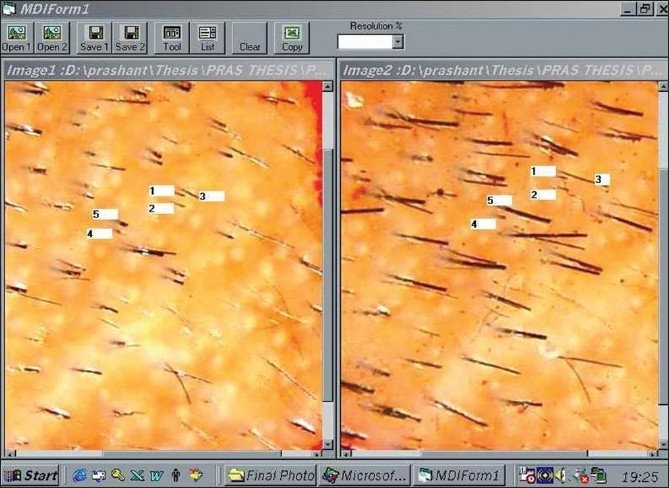
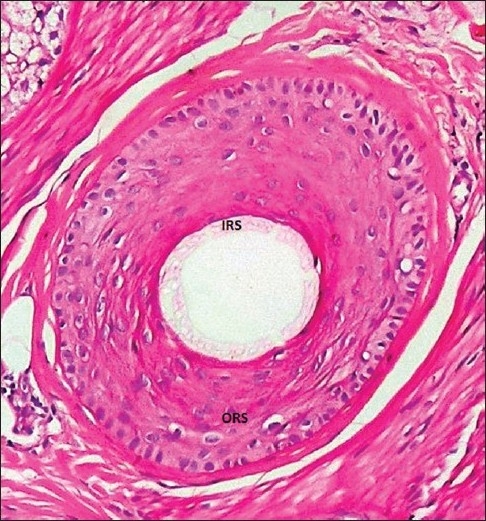
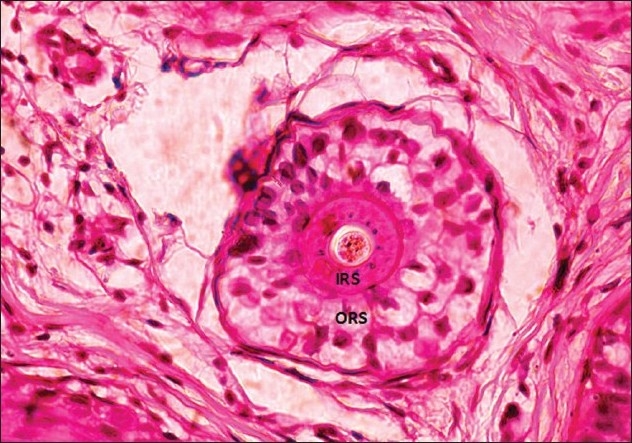
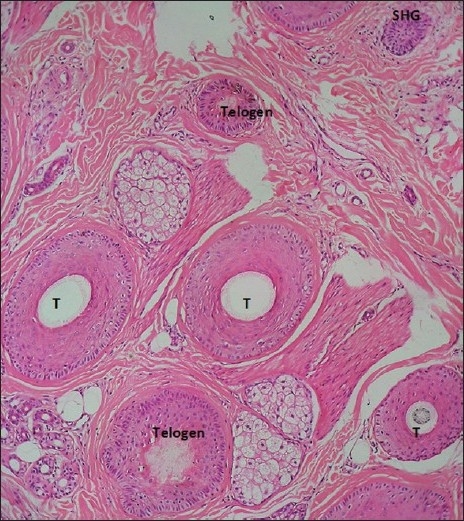
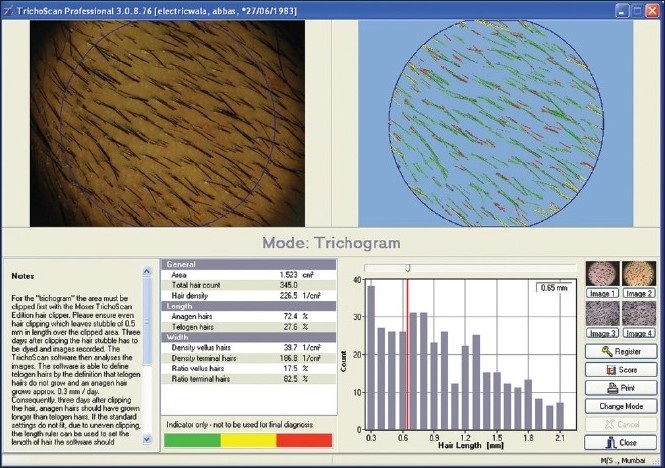
Various methods are available for evaluation (for diagnosis and/or quantification) of a patient presenting with hair loss. Hair evaluation methods are grouped into three main categories: Non-invasive methods (e.g., questionnaire, daily hair counts, standardized wash test, 60-s hair count, global photographs, dermoscopy, hair weight, contrasting felt examination, phototrichogram, TrichoScan and polarizing and surface electron microscopy), semi-invasive methods (e.g., trichogram and unit area trichogram) and invasive methods (e.g., scalp biopsy). Any single method is neither 'ideal' nor feasible. However, when interpreted with caution, these are valuable tools for patient diagnosis and monitoring. Daily hair counts, wash test, etc. are good methods for primary evaluation of the patient and to get an approximate assessment of the amount of shedding. Some methods like global photography form an important part of any hair clinic. Analytical methods like phototrichogram are usually possible only in the setting of a clinical trial. Many of these methods (like the scalp biopsy) require expertise for both processing and interpreting. We reviewed the available literature in detail in light of merits and demerits of each method. A plethora of newer methods is being introduced, which are relevant to the cosmetic industry/research. Such methods as well as metabolic/hormonal evaluation are not included in this review.
Keywords: Alopecia; diagnostic methods for hair loss; evaluating hair loss; hair loss; quantifying hair loss.
Conflict of interest statement
Figures







References
-
- Barber BL, Kaufman KD, Kozloff RC, Girman CJ, Guess HA. A hair growth questionnaire for use in the evaluation of therapeutic effects in men. J Dermatol Treat. 1998;9:181–6.
-
- The womens hair growth questionnaire: development and validation of a patient reported measure for treatment efficacy in androgenetic alopecia. J Am Acacd Dermatol. march 2009 (P2105)
-
- Shapiro J. Assessment of the patient with alopecia. In: Hair Loss., editor. Principles of Diagnosis and Management of alopecia. 1st ed. London: Martin Dunitz Ltd; 2002.
-
- Oslen E. Clinical tools for assessing hair loss. In: Oslen E, editor. Disorders of Hair growth Diagnosis and Treatment. New York: McGraw-Hill, Inc; 1994. pp. 59–69.
-
- Piérard GE, Piérard-Franchimont, Marks CR, Elsnerc P. EEMCO group. EEMCO Guidance for the Assessment of Hair Shedding and Alopecia. Skin Pharmacol Physiol. 2004;17:98–110. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
